Medial-Elbow Strain / Tendinopathy
- The FLEXOR-PRONATOR MASS is the common flexor-pronator origin from the MEDIAL EPICONDYLE (pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, flexor carpi ulnaris) and acts as an important DYNAMIC STABILISER against VALGUS stress at the elbow, helping to PROTECT the ULNAR COLLATERAL LIGAMENT (UCL) from injury.
- KNOW THE EPIDEMIOLOGY - THE TYPICAL PATIENT IS NOT AN ATHLETE. In a population study of 4,783 Finns aged 30 to 64, DEFINITE MEDIAL epicondylitis had a prevalence of 0.4 PERCENT against 1.3 PERCENT for LATERAL - so the medial form is roughly a THIRD as common, the single most quotable contrast between them. Prevalence did NOT differ between men and women and peaked at 45 to 54 YEARS. The throwing athlete is the memorable presentation, not the usual one.
- THERE ARE MODIFIABLE RISK FACTORS BEYOND SPORT. In that same population, SMOKING, OBESITY, REPETITIVE MOVEMENTS and FORCEFUL ACTIVITIES were each INDEPENDENTLY associated with medial epicondylitis - so smoking cessation, weight and an occupational-exposure history belong in the consultation alongside load management, and a patient whose work involves both repetition and force carries the highest exposure.
- Its injuries span: MEDIAL EPICONDYLITIS ('GOLFER'S/medial elbow') - a DEGENERATIVE TENDINOPATHY (angiofibroblastic change) of the origin, classically of the pronator teres/FCR portion; acute STRAIN; and, in THROWING athletes, repetitive valgus overload causing flexor-pronator STRAIN or PARTIAL TEARING/avulsion of the origin.
- The PRESENTATION is MEDIAL ELBOW PAIN aggravated by resisted wrist FLEXION and forearm PRONATION and by gripping, with tenderness over or just distal to the medial epicondyle; in throwers there is pain during late cocking/acceleration and loss of throwing velocity.
- The crucial clinical point is the MEDIAL-ELBOW TRIAD in the thrower: flexor-pronator injury must be DISTINGUISHED from UCL INJURY (which causes valgus instability - moving valgus stress test, MRI/arthrogram) and from ULNAR NEURITIS (ulnar nerve symptoms) - and these can COEXIST, because as a dynamic UCL backup the flexor-pronator is stressed alongside the ligament.
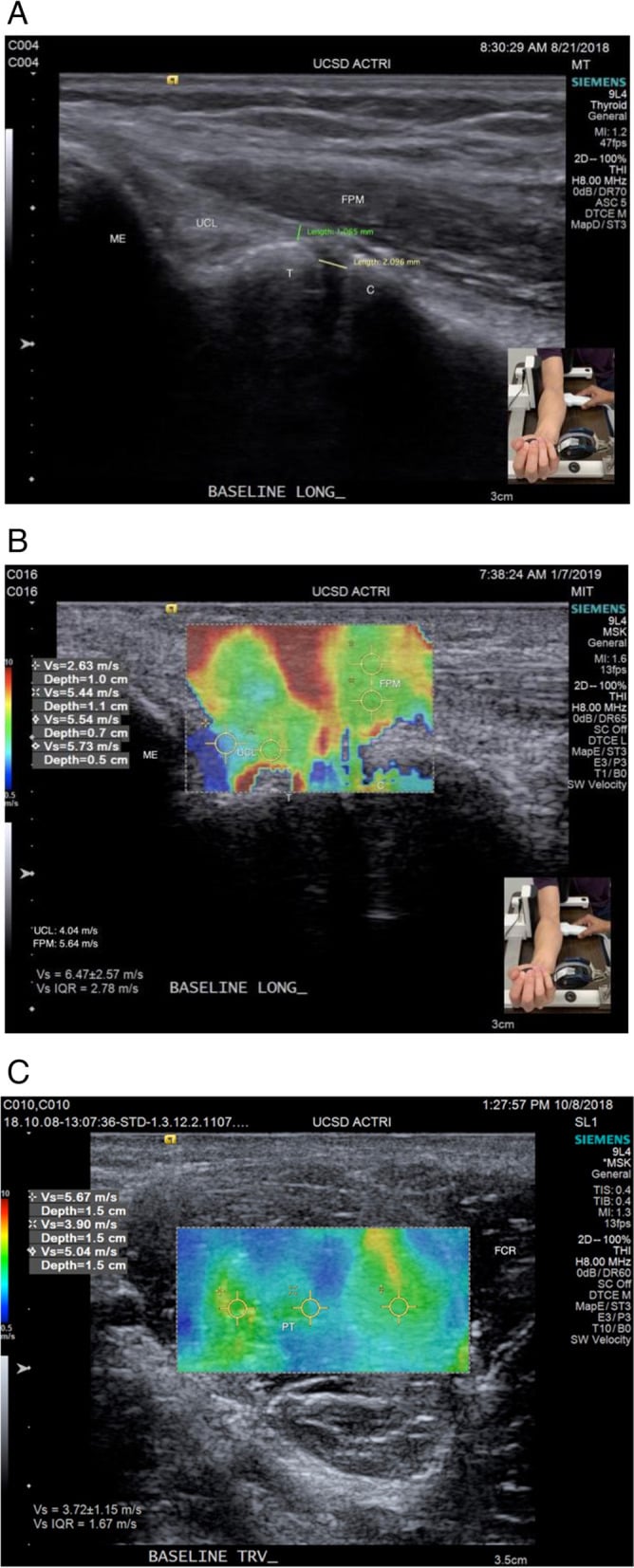
- DIAGNOSIS is clinical (site of tenderness, provocative resisted-flexion/pronation tests, valgus stability testing, ulnar nerve assessment) supported by IMAGING - ULTRASOUND/MRI to characterise the flexor-pronator tendinopathy/tear and to assess the UCL.
- MANAGEMENT is largely NON-OPERATIVE: relative REST/activity modification, ECCENTRIC and progressive loading REHABILITATION, NSAIDs, and a CAUTIOUS approach to corticosteroid injection (risk of tendon weakening); SURGERY (debridement of degenerate tendinopathy +/- repair/reattachment) is reserved for refractory cases - and in the thrower, any associated UCL insufficiency or ulnar neuritis must be addressed, because treating the flexor-pronator alone while missing UCL instability will fail.
- “Flexor-pronator mass = common flexor origin (medial epicondyle); a DYNAMIC valgus stabiliser that PROTECTS the UCL. Injuries: medial epicondylitis (golfer's elbow), strain, and throwers' partial tear/avulsion.
- “Presentation: medial elbow pain worse on resisted wrist FLEXION/PRONATION + gripping; throwers lose velocity. KEY: the medial-elbow TRIAD - distinguish (and look for coexisting) UCL injury (valgus instability) + ulnar neuritis.
- “Management mostly NON-OPERATIVE (rest, eccentric loading, NSAIDs; cautious injection); surgery (debridement +/- repair) for refractory cases. In throwers, address any UCL insufficiency/ulnar neuritis - don't treat the flexor-pronator in isolation.
- “Epidemiology is a favourite contrast: definite MEDIAL epicondylitis 0.4% vs LATERAL 1.3% in a 4,783-person population sample - about a THIRD as common; no sex difference; peak at 45-54 years. Independent risk factors are SMOKING, OBESITY, repetitive movements and forceful activities, so the commonest patient is a middle-aged worker, not an athlete.
Medial elbow pain worse on resisted wrist flexion/pronation + gripping, tender over the medial epicondyle = flexor-pronator strain/medial epicondylitis. A dynamic valgus stabiliser (protects the UCL).
UCL injury (valgus instability - moving valgus stress test/MRI) and ulnar neuritis. In throwers these coexist - treating the flexor-pronator alone while missing UCL instability fails.
Anatomy, Injury Spectrum & The Triad
The flexor-pronator mass (common flexor origin from the medial epicondyle) is a dynamic stabiliser to valgus stress that protects the UCL. Its injuries are medial epicondylitis ('golfer's elbow' - a degenerative tendinopathy, especially of the pronator teres/FCR), acute strain, and, in throwers, valgus- overload partial tearing/avulsion of the origin. Presentation is medial elbow pain worse on resisted wrist flexion/forearm pronation and gripping, with medial-epicondylar tenderness; throwers lose velocity. The crucial point is the medial-elbow triad: distinguish flexor-pronator injury from UCL injury (valgus instability) and ulnar neuritis - which often coexist in the thrower.
- Key feature
- Pain on resisted wrist flexion/pronation + gripping
- Test/clue
- Tender at/just distal to medial epicondyle
- Key feature
- Valgus instability; medial pain in late cocking
- Test/clue
- Moving valgus stress test; MRI/MR-arthrogram
- Key feature
- Ulnar nerve symptoms (little/ring finger, intrinsics)
- Test/clue
- Tinel's at cubital tunnel; nerve conduction
The Layered Anatomy and Innervation
- The layered origin. From the common flexor origin at the medial epicondyle, the superficial muscles lie (radial→ulnar) pronator teres → FCR → palmaris longus → FCU, with flexor digitorum superficialis forming an intermediate layer deep to them (also arising from the medial epicondyle plus the ulna/radius).
- The innervation. The median nerve supplies pronator teres, FCR, palmaris longus and FDS; the ulnar nerve supplies only the flexor carpi ulnaris of the origin - so FCU is the odd one out.
- The two nerves' relations. The median nerve passes between the two heads of pronator teres (the site of pronator syndrome); the ulnar nerve passes posterior to the medial epicondyle (cubital tunnel) then between the two heads of FCU - which is why medial-epicondylar pathology and its treatment sit so close to the ulnar nerve.
Q: What is the layered anatomy and innervation of the flexor-pronator mass?
A: From the common flexor origin (medial epicondyle), the superficial muscles lie radial→ulnar: pronator teres → FCR → palmaris longus → FCU, with FDS as an intermediate layer. Innervation: the median nerve supplies pronator teres/FCR/palmaris longus/FDS; the ulnar nerve supplies only the FCU. The median nerve passes between the two heads of pronator teres (pronator syndrome); the ulnar nerve passes posterior to the medial epicondyle (cubital tunnel) then between the two FCU heads - hence its proximity to medial-epicondylar pathology/surgery.
How the Flexor-Pronator Protects the UCL (and Its Limit)
- How it protects the UCL. The flexor-pronator muscles - especially FCU and FDS, which overlie the anterior band of the UCL - contract during valgus load and generate a compressive/medial force that shares the valgus load, reducing the tension the UCL must bear and limiting ulnohumeral joint-space gapping; grip and pronation increase this activation. So the flexor-pronator is a dynamic backup to the static UCL.
- Its limit. The protection is not constant - it depends on elbow flexion angle and load, and at the very high valgus torques of pitching (which approach or exceed the UCL's failure load) the dynamic contribution may be less protective than once believed. So the flexor-pronator cannot substitute for a competent UCL - the clinical reason a flexor-pronator injury with underlying UCL insufficiency will not settle until the ligament is addressed.
Q: How does the flexor-pronator mass protect the UCL biomechanically, and what is the limit?
A: During valgus load the flexor-pronator muscles - especially FCU and FDS overlying the anterior band of the UCL - contract and generate a compressive/medial force that shares the valgus load, reducing UCL tension and ulnohumeral joint-space gapping (grip + pronation increase this) - a dynamic backup to the static UCL. But the protection is position/load-dependent: at the very high valgus torques of pitching it may be less protective than believed, so the flexor-pronator cannot substitute for a competent UCL (hence a flexor-pronator injury with UCL insufficiency will not settle until the ligament is fixed).
Who Actually Gets This - the Population Numbers
The throwing athlete is the teaching case, but not the typical patient. In a population sample of 4,783 people aged 30 to 64 in Finland (81.5 percent of those invited), the prevalence of definite medial epicondylitis was 0.4 percent against 1.3 percent for lateral - so the medial form is roughly a third as common, which is the contrast worth being able to quote. Prevalence did not differ between men and women and was highest at 45 to 54 years. That matters clinically as well as for the exam: a middle-aged manual worker with medial elbow pain is the commoner presentation, and the medial-elbow triad framing belongs to the thrower rather than to everyone with a tender medial epicondyle.
In that population, smoking, obesity, repetitive movements and forceful activities were each independently associated with medial epicondylitis. So the consultation should include an occupational exposure history, smoking cessation and weight, not only load management - and for lateral epicondylitis the interaction between repetition and force was striking (odds ratio 5.6 for both together against neither), which is the pattern to ask about.
This is a cross-sectional survey, so the associations are not proof that stopping smoking or losing weight resolves the tendinopathy - no trial has tested that. It also counted epicondylitis, not flexor-pronator tearing in throwers, so it says nothing about the prevalence of partial origin tears in that group, and the single-country sample may not transfer to other working populations.
Management
- Non-operative (mainstay): relative rest/activity modification, eccentric and progressive loading rehabilitation, NSAIDs; cautious corticosteroid injection (tendon-weakening risk).
- Address the triad (throwers): assess and treat any coexisting UCL insufficiency (the dynamic stabiliser cannot compensate for an incompetent ligament) and ulnar neuritis.
- Surgery (refractory): debridement of degenerate tendinopathy +/- repair/reattachment of a torn origin; UCL reconstruction if the ligament is insufficient.
- Address the risk factors, not only the load: smoking and obesity were independently associated with medial epicondylitis in population data, alongside repetitive and forceful work - so take an occupational history and raise both, while noting that no trial has shown modifying them resolves the tendinopathy.
- Return to throwing: graded, with attention to mechanics/kinetic chain and workload.
The three medial-elbow problems each have their own page, and in the thrower they must be assessed together: ulnar collateral ligament injury, the tendinopathy itself under medial epicondylitis, and the nerve under cubital tunnel syndrome. The lateral counterpart, three times commoner in the population, is lateral epicondylitis, and in the skeletally immature the same valgus mechanism avulses bone rather than tendon - see medial epicondyle fractures.
The most important clinical caution with flexor-pronator mass injury is in the throwing athlete, where the medial elbow harbours a triad of overlapping problems - flexor-pronator strain/tendinopathy, ulnar collateral ligament injury, and ulnar neuritis - that frequently coexist. This is not coincidental: the flexor-pronator mass is a dynamic stabiliser against valgus and backs up the UCL, so the repetitive valgus loads of throwing stress both the muscle origin and the ligament together. The error to avoid is diagnosing and treating an apparent flexor-pronator strain or medial epicondylitis while missing underlying UCL insufficiency - because a dynamic stabiliser cannot compensate for an incompetent ligament, and the athlete will not return to throwing until the ligament is addressed. So the medial elbow should be assessed comprehensively: provocative resisted-flexion/pronation testing for the flexor-pronator, valgus stability testing (e.g. the moving valgus stress test) and MRI for the UCL, and ulnar nerve assessment. Most isolated flexor-pronator injuries respond to non-operative rehabilitation, with surgery reserved for refractory cases, and corticosteroid injection used cautiously given the tendon-weakening risk.
Mnemonics & Memory Aids
MEDIAL
Hook:MEDIAL: Medial epicondyle (valgus stabiliser), Epicondylitis/strain/tear, Distinguish the triad, Investigate (valgus/UCL/nerve), Address UCL insufficiency, Load rehab first.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A baseball pitcher has medial elbow pain and tenderness over the flexor-pronator origin. Why must you not stop at diagnosing flexor-pronator strain?”
Anatomy & function
- Common flexor-pronator origin (medial epicondyle): PT, FCR, PL, FDS, FCU
- Dynamic stabiliser to valgus stress - protects the UCL
- Protection is position/load dependent
Injury spectrum & presentation
- Medial epicondylitis (golfer's elbow) - prevalence 0.4 percent, a third that of lateral (1.3 percent); peak 45-54, no sex difference
- Strain and throwers' partial tear/avulsion; risk factors include smoking, obesity, repetitive and forceful work
- Medial elbow pain worse on resisted wrist flexion/pronation + gripping
- Throwers: pain in late cocking/acceleration; loss of velocity
The medial triad
- Flexor-pronator injury + UCL injury + ulnar neuritis (coexist)
- Test: resisted flexion/pronation; moving valgus stress test/MRI; ulnar nerve
- Don't treat the flexor-pronator in isolation (miss UCL insufficiency)
Management
- Non-operative: rest, eccentric/progressive loading, NSAIDs; cautious injection
- Surgery (debridement +/- repair) for refractory cases
- Address UCL insufficiency (reconstruction) / ulnar neuritis; graded return to throwing
Evidence & Key Studies
The flexor-pronator mass as a dynamic stabiliser of the medial elbow (and UCL protection)
- The flexor-pronator mass is an important dynamic stabiliser against valgus stress at the elbow and has been reported to protect against ulnar collateral ligament injury.
- Active gripping and pronation have been shown to reduce ulnohumeral joint space and alter ligament material properties, reflecting the flexor-pronator's contribution to medial-elbow stability.
- The protective effect of flexor-pronator activation may be joint-position or load dependent (it may not be as protective during the very high valgus stress of pitching as believed) - underscoring its role and limits as a dynamic UCL backup.
Prevalence and determinants of lateral and medial epicondylitis: a population study
- Representative population sample of people aged 30 to 64 living in Finland in 2000 to 2001: 4,783 of 5,871 invited (81.5 percent) were included and examined.
- Prevalence of definite lateral epicondylitis was 1.3 percent and of definite medial epicondylitis 0.4 percent - the medial form roughly a third as common. Prevalence did not differ between men and women and was highest at 45 to 54 years.
- Smoking, obesity, repetitive movements and forceful activities were each independently associated with medial epicondylitis. For lateral epicondylitis, current smoking carried an odds ratio of 3.4 and there was a significant interaction between repetitive and forceful activity (odds ratio 5.6 for both versus neither). The design is cross-sectional, so these are associations rather than demonstrated causes, and the sample is from one country.
The role of the flexor-pronator mass as an important dynamic stabiliser against valgus stress at the elbow that helps protect the ulnar collateral ligament (and the position/load dependence of this protection) comes from the cited Gong study. The spectrum of flexor-pronator injury (medial epicondylitis/golfer's elbow, strain, throwers' partial tear), the medial-elbow triad with UCL injury and ulnar neuritis, the provocative examination, and the non-operative-first management (with surgery for refractory cases and addressing coexisting UCL insufficiency) are standard, well-established teaching. The prevalence figures, the age and sex distribution and the independent risk factors come from the Shiri population study, which is cross-sectional and Finnish, so the associations are not demonstrated causes and no trial has tested whether modifying smoking or weight resolves the tendinopathy. No study gives the prevalence of flexor-pronator partial tearing in throwers, no trial compares eccentric loading, injection and surgery for medial epicondylitis, and no validated return-to-throwing timeline exists - so none is quoted here.