Neuropathic Arthropathy of the Glenohumeral Joint
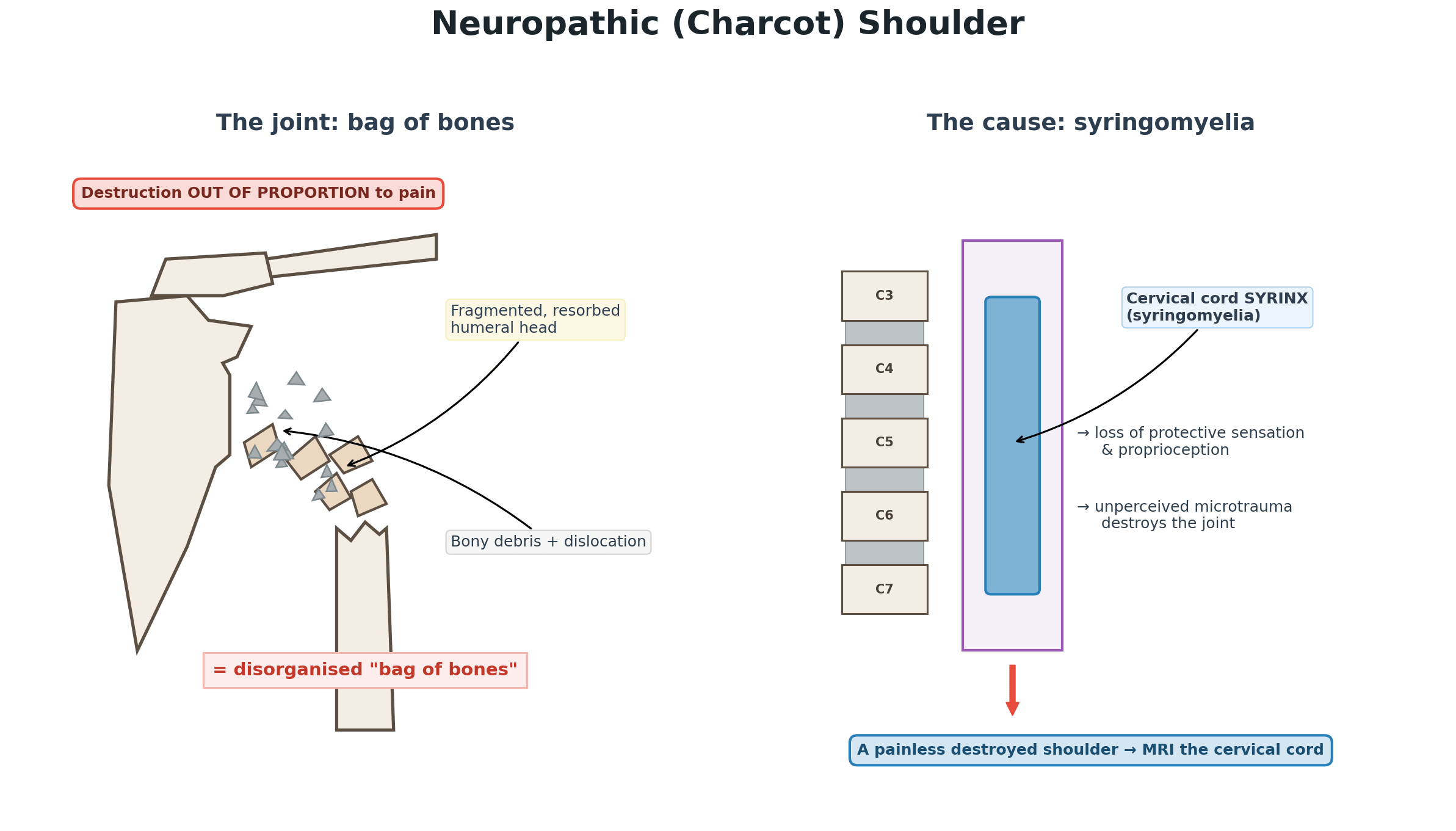
- Charcot (neuropathic) arthropathy of the shoulder is a progressive, grossly destructive arthropathy in which the joint destruction is OUT OF PROPORTION to the pain - the hallmark is a markedly swollen, often unstable shoulder with surprisingly LITTLE pain, because the underlying problem is loss of protective sensation and proprioception.
- SYRINGOMYELIA is the leading cause of an upper-limb (elbow and shoulder) neuropathic joint, so a painless destroyed shoulder should prompt MRI of the CERVICAL SPINAL CORD to look for a syrinx (often associated with a Chiari malformation); other causes include cervical cord lesions and peripheral neuropathies.
- The pathophysiology combines the NEUROTRAUMATIC theory (loss of protective sensation allows repetitive unperceived microtrauma and progressive destruction) and the NEUROVASCULAR theory (autonomic dysregulation increasing blood flow and bone resorption); the result is fragmentation, resorption and disorganisation of the joint.
- RADIOGRAPHS show gross destruction - resorption and fragmentation of the humeral head, bony debris and a disorganised 'BAG OF BONES' appearance - and the classic teaching summarises the changes as the 6 Ds (Destruction, Density increase/sclerosis, Debris, Dislocation, Disorganisation, Distension); the shoulder is often grossly swollen with effusion.
- The crucial step is the DIFFERENTIAL: the swollen, destroyed, fluid-filled shoulder can mimic a soft-tissue or bone TUMOUR (an expansile mass) or INFECTION (septic arthritis/osteomyelitis), so these must be excluded with appropriate imaging and, when there is doubt, aspiration and/or biopsy, before the destruction is attributed to a neuropathic process.
- Management is largely SUPPORTIVE - treat the underlying neurological cause (e.g. neurosurgical decompression of a syrinx where indicated), protect the joint, and manage symptoms - because surgery on a Charcot joint has high complication and failure rates; arthrodesis is difficult and unreliable, and arthroplasty is reserved for carefully selected cases, ideally after the neurological process is addressed and within a multidisciplinary team.
- “Charcot shoulder = PAINLESS gross destruction (destruction out of proportion to pain) - think SYRINGOMYELIA; image the cervical cord (MRI).
- “Radiograph: 'bag of bones' - the 6 Ds (Destruction, Density, Debris, Dislocation, Disorganisation, Distension).
- “Always exclude TUMOUR and INFECTION first; management mainly supportive + treat the cause; surgery is unreliable and selective.
A grossly swollen, destroyed, often unstable shoulder with surprisingly little pain - destruction out of proportion to symptoms. Radiograph: 'bag of bones'.
Think syringomyelia - MRI the cervical cord. And exclude tumour and infection before calling it neuropathic.
Pathophysiology, Cause & Radiology
The defining feature of a Charcot shoulder is destruction out of proportion to pain: the joint is grossly swollen and disorganised, often unstable, yet relatively painless, because the underlying problem is loss of protective sensation and proprioception. The leading cause of an upper-limb neuropathic joint (elbow and shoulder) is syringomyelia, so a painless destroyed shoulder should prompt MRI of the cervical spinal cord to find a syrinx. The mechanism combines the neurotraumatic theory (unperceived repetitive microtrauma) and the neurovascular theory (autonomic dysregulation increasing bone resorption). Radiographs show resorption and fragmentation of the humeral head with bony debris - the disorganised 'bag of bones', summarised as the 6 Ds (Destruction, Density, Debris, Dislocation, Disorganisation, Distension).
The bedside sign that makes the diagnosis is the sensory pattern, not the joint. A cervical syrinx expands first through the crossing spinothalamic fibres in the anterior commissure, so it produces dissociated sensory loss - pain and temperature sensation are lost while light touch, vibration and proprioception are preserved - distributed over the shoulders and upper trunk in the classic "cape" or "shawl" distribution. Look also for wasting and weakness of the small muscles of the hand (anterior horn involvement) and lost upper-limb reflexes. A patient who cannot feel a pinprick over the shoulder but can feel light touch there has declared the cause of their destroyed joint.
Atrophic versus hypertrophic. Charcot joints take two radiographic forms, and the limb predicts which. The upper limb, and syringomyelic joints in particular, tend to the ATROPHIC pattern - pure osteolysis and resorption of the humeral head with little new bone, so the head appears to dissolve or be "licked" away. The hypertrophic pattern - exuberant sclerosis, osteophyte and periosteal new bone, the full 6 Ds - is more characteristic of the weight-bearing lower limb, as in the diabetic Charcot foot. Expect resorption at the shoulder and do not be reassured by the absence of florid new bone.
Causes of a Neuropathic Joint: Which Disease, Which Joint
Syringomyelia is the classic upper-limb cause, but the joint distribution usually points to the underlying neurological disease (each cause is developed in its own topic).
- Typical joint(s)
- UPPER LIMB - shoulder and elbow
- The investigation that identifies it
- MRI of the cervical cord and craniocervical junction - the single most important test in a destroyed shoulder
- Typical joint(s)
- FOOT and ankle (commonest cause overall)
- The investigation that identifies it
- Glucose and HbA1c with bedside sensory testing (monofilament, vibration)
- Typical joint(s)
- KNEE, hip and spine (large lower-limb joints)
- The investigation that identifies it
- Treponemal serology - rare now, but the classic answer and a treatable cause
- Typical joint(s)
- Hands and feet
- The investigation that identifies it
- Slit-skin smear and nerve examination for thickened peripheral nerves; consider in endemic or migrant populations
- Typical joint(s)
- Lower limb and spine (below the level)
- The investigation that identifies it
- The history gives it; image the cord if the level or function has changed
- Typical joint(s)
- Feet (hereditary neuropathy); the injected joint (steroid)
- The investigation that identifies it
- Family history with nerve conduction studies; a drinking history; a record of injections
Each of these is developed separately in syringomyelia, Chiari malformation, Charcot neuroarthropathy, diabetic neuropathy, spinal cord injury, myelomeningocele, hereditary motor and sensory neuropathies and, for the elbow, Charcot neuropathic joint of the elbow.
Let the joint point to the cause: a destroyed UPPER-LIMB joint (shoulder/elbow) = syringomyelia until proven otherwise (MRI the cervical cord); foot/ankle = diabetes (commonest overall); knee/hip = tabes dorsalis classically. Leprosy, spinal cord injury, hereditary sensory neuropathies, alcohol and repeated intra-articular steroid are the other recognised causes.
Differential & Management
- Exclude the dangerous mimics first. The grossly swollen, destroyed, fluid-filled shoulder can look like a tumour (an expansile mass) or infection (septic arthritis/osteomyelitis); image appropriately and, when there is doubt, aspirate and/or biopsy before attributing the destruction to neuropathy. Note that infection can coexist with a neuropathic joint rather than merely mimic it, so a raised inflammatory response does not exclude the diagnosis - and does not excuse skipping the aspirate.
- The other destroyed shoulder to know is Milwaukee shoulder - rapidly destructive cuff-tear arthropathy driven by basic calcium phosphate crystals, in an elderly patient with a large effusion and a massive cuff tear. It is distinguished by the absence of a neurological deficit and by pain that fits the destruction, whereas the Charcot shoulder is painless out of proportion (developed in our Milwaukee Shoulder and Rotator Cuff Arthropathy topics).
- Find and treat the underlying cause. Image the cervical cord (MRI) for a syrinx (often with a Chiari malformation); neurosurgical decompression may be indicated for a progressive syrinx.
- Largely supportive joint care. Protect the joint, manage symptoms and maintain function; activity modification and bracing have a role.
- Surgery is selective and unreliable. Charcot joints have high surgical complication and failure rates; arthrodesis is difficult and often fails, and arthroplasty is reserved for carefully selected cases, ideally after the neurological process is addressed, within a multidisciplinary team.
The two classic errors with a Charcot shoulder are at opposite ends. The first is mistaking the swollen, fluid-filled, destroyed joint for a malignancy or an infection and either over-investigating destructively or missing a genuine concurrent tumour/sepsis - so the differential must be excluded with imaging and, when in doubt, aspiration/biopsy. The second is operating too readily: a neuropathic joint tolerates surgery poorly, arthrodesis frequently fails to fuse, and arthroplasty has high complication rates, so surgery is reserved for carefully selected cases and is best undertaken only after the underlying neurological cause has been addressed. The single most useful reflex is to recognise the dissociation between gross destruction and minimal pain and to image the cervical cord for a syrinx.
Surgery for the Neuropathic Shoulder: Options and Why They Fail
Surgery here is selective and unreliable, and both the reason and the available options are examinable (the procedures themselves are developed in our Shoulder Arthrodesis and Reverse Total Shoulder Arthroplasty topics).
- Why it fails. The 'bag of bones' gives poor bone stock for fixation or fusion; crucially the underlying neuropathy persists, so protective sensation is still absent and continued unperceived loading drives recurrent destruction, implant loosening and non-union; rates of infection and instability are high, and the painless instability is often surprisingly well tolerated.
- Largely non-operative. Protect the joint, modify activity, brace, control symptoms - the default.
- When surgery is considered. Intractable pain, gross instability or functional loss - and only after the neurological process has been addressed and is quiescent, within an MDT.
- The options. Resection arthroplasty; arthrodesis (technically difficult with a high non-union rate in the neuropathic joint); and arthroplasty - typically a constrained or reverse total shoulder replacement for the unstable, often cuff-deficient neuropathic shoulder - all with guarded outcomes and high complication rates. Counsel for function/symptom control, not a normal joint.
Surgery fails because the neuropathy persists (continued unperceived loading -> recurrent destruction, loosening, non-union) on poor bone stock, with high infection/instability. So default to supportive care; reserve surgery for intractable pain/instability only after the neurology is quiescent - options are resection, (often-failing) arthrodesis, or a constrained/reverse arthroplasty - and counsel realistically.
Mnemonics & Memory Aids
6 Ds
Hook:The 6 Ds of a Charcot joint: Destruction, Density, Debris, Dislocation, Disorganisation, Distension.
CHARCOT
Hook:CHARCOT: image the Cord, Hot/swollen but Absent pain, Resorption, exclude Cancer/infection, Operate selectively, Treat the cause.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a grossly swollen, destroyed shoulder on X-ray but very little pain. What is your diagnosis and what is the key investigation?”
“How would you manage a confirmed neuropathic shoulder due to syringomyelia?”
Recognition
- Gross destruction with little pain (destruction out of proportion to symptoms)
- Swollen, often unstable shoulder; radiograph 'bag of bones' / 6 Ds
- Mechanism: loss of protective sensation + proprioception (neurotraumatic + neurovascular)
Cause & key investigation
- Syringomyelia is the leading upper-limb cause (elbow and shoulder)
- MRI the cervical cord (syrinx, often with Chiari malformation)
- Also consider cervical cord lesions, peripheral neuropathy
Differential (exclude first)
- Tumour (expansile fluid-filled mass) - biopsy if doubt
- Infection (septic arthritis/osteomyelitis) - aspirate if doubt
- Do not attribute to neuropathy until mimics excluded
Management
- Largely supportive: protect joint, activity modification, bracing, symptom control
- Treat the cause (neurosurgical decompression of progressive syrinx)
- Surgery selective/unreliable (arthrodesis often fails; arthroplasty high risk); MDT
Evidence & Key Studies
Orthopedic manifestations of syringomyelia: a comprehensive review (with neuropathic shoulder case)
- Orthopaedic involvement in syringomyelia includes progressive spinal deformities (scoliosis, often with Chiari malformation) and neurogenic joint destruction, particularly affecting the shoulder and elbow.
- Charcot joints result from impaired proprioception and protective sensation; these orthopaedic complications may be early diagnostic clues yet are often under-recognised.
- Conservative treatment is the mainstay in stable cases, with surgery reserved for progressive disease; early recognition and multidisciplinary management prevent irreversible sequelae.
Neuropathic arthropathy of the shoulder in chronic syrinx mimicking malignancy
- Syringomyelia is a prevalent cause of Charcot arthropathy, notably affecting the elbow and less frequently the shoulder.
- Shoulder neuropathic arthropathy can present as an expansile fluid-filled mass with significant bone destruction, raising suspicion of malignancy - bone biopsy was needed to exclude tumour.
- Diagnosis relies on clinical signs, imaging and exclusion of other causes (including soft-tissue tumours); management spans conservative care to neurosurgical decompression and shoulder arthroplasty, within a multidisciplinary approach.
The link between syringomyelia and neurogenic destruction of the shoulder and elbow, the mechanism (impaired proprioception and protective sensation), and the conservative-mainstay/surgery-for- progressive-disease approach come from the cited Fadila review; the fact that syringomyelia is a prevalent cause of Charcot arthropathy, that the shoulder can present as an expansile fluid-filled mass mimicking malignancy requiring biopsy to exclude tumour, and the management spectrum (conservative to neurosurgical decompression and arthroplasty) from the cited Edara case report. The neurotraumatic/neurovascular pathophysiology and the radiographic '6 Ds / bag of bones' description are standard, well-established teaching. (See also our Charcot Neuroarthropathy and Septic Arthritis topics.)