An Overuse Injury of the Throwing Elbow
- Olecranon stress fracture is an OVERUSE injury that primarily affects THROWING athletes (baseball pitchers, javelin) and athletes exposed to high repetitive compressive loads such as gymnasts; the incidence is rising with year-round youth sport, so it should be considered in any thrower with persistent posterior elbow pain.
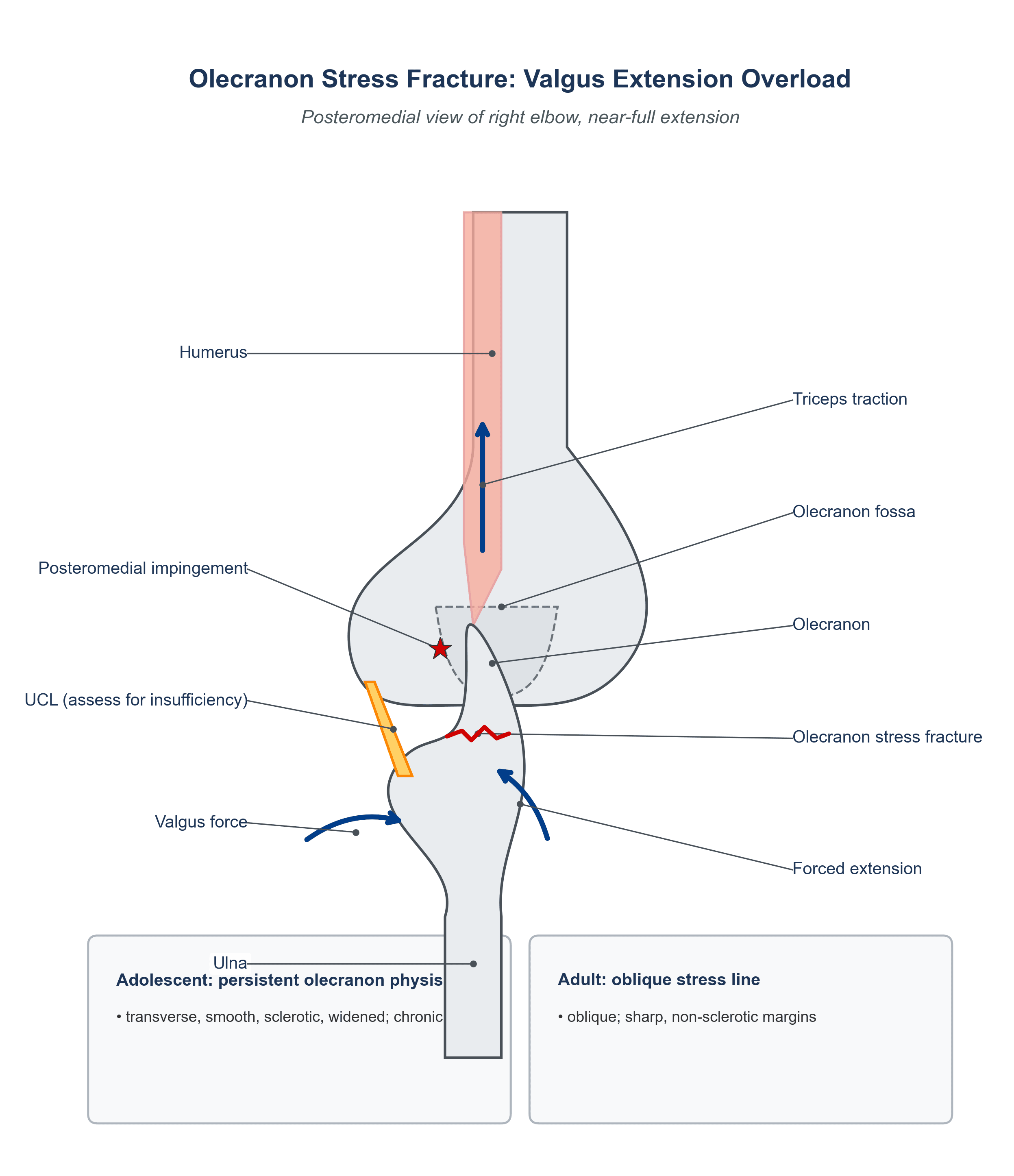
- The mechanism is VALGUS EXTENSION OVERLOAD: repetitive forced elbow extension combined with valgus stress during the throwing motion drives the olecranon against the olecranon fossa (posteromedial impingement) and applies repetitive triceps traction, so the posteromedial olecranon is loaded cyclically until a stress reaction and then a stress fracture develop.
- The presentation is POSTERIOR elbow pain that is worse on extension and with throwing (and may be associated with reduced velocity/performance); examination shows posterior/posteromedial tenderness and pain on forced extension, and there may be signs of associated valgus extension overload such as a posteromedial osteophyte.
- There are two recognised PATTERNS: in the skeletally immature, a PERSISTENT (non-united, widened) OLECRANON PHYSIS - effectively a physeal stress injury that fails to fuse - and in the adult, an OBLIQUE STRESS FRACTURE LINE through the olecranon; recognising which pattern is present guides treatment.
- Plain radiographs are often NORMAL early, so MRI (showing marrow oedema/stress reaction before a line is visible) or CT is frequently required for definitive diagnosis; it is also essential to assess for VALGUS INSTABILITY and ulnar collateral ligament (UCL) insufficiency, because UCL laxity increases posteromedial load and an unaddressed UCL problem predisposes to recurrence.
- MANAGEMENT is REST and activity modification for early stress reactions and many fractures, but advanced or established pathology - a persistent physis or a complete/non-union stress fracture, or the need to return an ELITE thrower reliably - often requires SURGICAL FIXATION (a tension-band construct or, commonly in throwers, an intramedullary compression SCREW, with bone grafting for non-union), together with addressing any UCL/valgus instability.
- “Olecranon stress fracture = overuse in THROWERS (and gymnasts) via VALGUS EXTENSION OVERLOAD; posterior elbow pain worse on extension.
- “Two patterns: adolescent PERSISTENT OLECRANON PHYSIS vs adult OBLIQUE stress line; plain films often normal early -> MRI/CT.
- “Always assess UCL/valgus instability; rest for early, surgical fixation (tension band or intramedullary screw) for established/non-union or elite return.
A thrower with posterior elbow pain worse on extension; valgus extension overload. Plain films may be normal - get an MRI/CT.
Assess the UCL / valgus instability - posteromedial overload and recurrence relate to it, and it may need treating alongside the fracture.
Mechanism, Patterns & Diagnosis
Olecranon stress fracture is an overuse injury of throwing athletes (and gymnasts) produced by valgus extension overload: repetitive forced elbow extension with valgus drives the olecranon against its fossa (posteromedial impingement) and applies cyclical triceps traction until a stress reaction and then a fracture develop. The patient has posterior elbow pain that is worse on extension and with throwing, with posteromedial tenderness. There are two patterns - the adolescent persistent (non-united) olecranon physis and the adult oblique stress line. Plain radiographs are often normal early, so MRI (marrow oedema) or CT confirms the diagnosis, and it is essential to assess for valgus instability / UCL insufficiency, which loads the posteromedial elbow and predisposes to recurrence if unaddressed.
Differential Diagnosis of Posterior Elbow Pain in the Thrower
Posterior elbow pain in a thrower has a short, examinable differential - and the entities co-exist, because the same valgus extension overload that stress-fractures the olecranon also produces the posteromedial osteophyte and loads the UCL. Finding one does not exclude the others, and each is developed in its own right in Valgus Extension Overload of the Elbow, Elbow UCL Injury, Triceps Tendon Rupture, Snapping Triceps Syndrome, Olecranon Fractures and Little League Elbow. The discriminators are the precise site of tenderness, what provokes the pain, and any mechanical or neurological symptoms.
- Discriminating feature
- Posteromedial pain worse on terminal extension and throwing; insidious overuse onset
- Key test / finding
- Films often normal early; MRI marrow oedema / CT stress line
- What it means for management
- Rest, or fixation for established disease
- Discriminating feature
- Painful catching/locking in terminal extension; posteromedial olecranon osteophyte
- Key test / finding
- Valgus extension snap (overload) test; osteophyte on films/CT
- What it means for management
- Debride the osteophyte only after assessing the UCL - resecting too much olecranon increases valgus strain and can precipitate UCL failure
- Discriminating feature
- MEDIAL (not posterior) pain, loss of velocity, sense of instability
- Key test / finding
- Moving valgus stress test; valgus laxity; MRI/MR-arthrogram of UCL
- What it means for management
- Rehabilitation for the recreational thrower; reconstruction for the overhead athlete who needs velocity - and it commonly coexists with olecranon stress injury, so look for both
- Discriminating feature
- Pain localised to the triceps insertion, worse on RESISTED extension
- Key test / finding
- Tenderness at the insertion; tendinosis/partial tear on MRI
- What it means for management
- Load-based rehabilitation for tendinopathy; repair for a substantial partial or complete tear, since triceps insufficiency costs active extension
- Discriminating feature
- Medial snapping with elbow flexion; ulnar nerve paraesthesiae
- Key test / finding
- Palpable snapping of the medial triceps/ulnar nerve; positive Tinel
- What it means for management
- A nerve problem, not a bone one - and transposing the ulnar nerve without addressing a snapping medial triceps head leaves the snapping behind
- Discriminating feature
- Acute traumatic event (fracture) or fluctuant posterior swelling (bursitis)
- Key test / finding
- Sharp non-sclerotic fracture line; clinical fluctuant bursa
- What it means for management
- An acute fracture is fixed on its own merits; a bursitis is managed non-operatively once infection is excluded. Neither needs the throwing-load analysis this page is about
- Discriminating feature
- MEDIAL apophyseal pain in the skeletally immature thrower
- Key test / finding
- Medial apophyseal tenderness/widening (vs the posterior olecranon physis)
- What it means for management
- Rest from throwing and a pitch-count limit - in the skeletally immature the apophysis is the weak link, so the same load that stress-fractures an adult olecranon injures the growth centre instead
The Persistent Olecranon Physis: Ossification and Telling It From a Fracture
The adolescent pattern - the "persistent olecranon physis" - is best understood from the normal ossification timetable. The olecranon secondary ossification centre is one of the later elbow centres: it typically appears around age 8 to 10 years and fuses by approximately age 14 to 16 years (girls generally earlier than boys). In a symptomatic adolescent thrower, an olecranon physis that remains open and widened beyond the expected age of fusion is not a normal variant but a chronic physeal stress injury - the repetitive triceps traction and valgus extension overload prevent the apophysis from uniting, analogous to a chronic physeal (Salter-Harris-type) stress lesion. Comparison radiographs of the contralateral elbow are useful, because the asymptomatic side is usually fused or fusing while the symptomatic physis stays open and widened.
A transverse, smooth, sclerotic, widened lucency along the physeal line, with chronic sclerotic margins and an insidious overuse history. It behaves like a non-union: if it will not unite with rest it commonly needs fixation (intramedullary screw plus or minus grafting).
A sharp, irregular, non-sclerotic lucency with a clear traumatic event. Its classification and fixation (tension band, plate) are a separate problem - see Olecranon Fractures - and the distinction matters because it drives whether you are treating a fresh injury or a failed-to-unite physis.
The single best discriminator of the adolescent persistent physis from an acute fracture is the margin: a persistent physis is smooth and sclerotic (chronic), an acute fracture is sharp and non-sclerotic. Bilateral films and the history (insidious overuse vs a discrete injury) seal it.
The UCL Runs Both Ways - and the Trap Is in the Second Direction
Valgus instability and posteromedial olecranon overload are linked in both directions, and the second one is where surgeons cause harm.
Direction one, the familiar one. The anterior bundle of the ulnar collateral ligament is the primary restraint to valgus. When it attenuates, valgus opening increases, the olecranon tip is driven earlier and harder into the medial wall of its fossa, and the posteromedial bone is loaded beyond what it can remodel. UCL insufficiency therefore causes olecranon overload, which is why it must be sought in every case and treated where present.
Direction two, the one that gets missed. Once a posteromedial osteophyte has formed, it acts as a secondary stabiliser against valgus - a bony block substituting for the ligament that is failing. Removing it without addressing the UCL takes away that substitute restraint and can precipitate frank valgus instability. The same logic applies to bone resected beyond the osteophyte: resect only back to the anatomic olecranon contour, because normal olecranon removed in the belief that more decompression is better converts an impingement problem into an instability problem.
- What to do
- Clinical valgus and moving valgus stress testing, plus MRI or MR arthrogram
- Why
- The decision to debride depends on ligament competence; a lax UCL changes the operation
- What to do
- Define the anatomic contour on imaging before theatre, not by eye at arthroscopy
- Why
- The osteophyte blends into normal bone, and the transition is hard to judge intraoperatively
- What to do
- Take the osteophyte, not the olecranon
- Why
- Bone beyond the osteophyte is a valgus restraint - removing it increases UCL strain
- What to do
- Address the ligament in the same setting rather than deferring
- Why
- Debriding a stabiliser away from an incompetent ligament is the mechanism of iatrogenic instability
- What to do
- Leaving a small residual osteophyte is the safer error
- Why
- Residual impingement can be revised; a destabilised elbow in a thrower may not be recoverable
The full decompression technique, its resection limits and the instability complication are set out in Valgus Extension Overload of the Elbow, and ligament assessment and reconstruction in Elbow UCL Injury - the same rule appears in all three because it is the single commonest way a throwing elbow is made worse by an operation.
Management
- Rest and activity modification for stress reactions and many stress fractures - a structured throwing programme guides graded return to play.
- Surgical fixation for advanced/established pathology - a persistent olecranon physis, a complete or non-union stress fracture, or to reliably return an elite thrower: a tension-band construct or, commonly in throwers, an intramedullary compression screw, with bone grafting for non-union.
- Address valgus instability / UCL. Because UCL insufficiency increases posteromedial load, evaluate and, where indicated, treat (UCL reconstruction) to prevent recurrence.
- Prevent recurrence. Manage throwing volume/mechanics; persistent or recurrent pain warrants re-evaluation for non-union or unrecognised valgus instability.
Judging union: the plain film will mislead you in both directions. The stress line lies in a plane the lateral radiograph presents obliquely and the olecranon is a dense, superimposed structure, so a film can show an apparently persistent line in a healed bone and a healed-looking bone in a persistent non-union. Union is assessed on CT, which shows bridging trabeculae across the fracture plane, and this matters because the decision being made is whether to let an athlete resume the exact load that broke the bone. Radiographic appearance alone should not release a thrower back to throwing.
Return is criterion-based, not calendar-based. A time interval is a poor instrument here: healing rates vary, the underlying literature is small case series rather than trials, and a date on a calendar tells you nothing about the bone. Progress through the following, and stop and reassess if pain returns at any stage:
- What must be true
- No pain at rest, no posterior elbow pain on forced terminal extension, and no tenderness over the posteromedial olecranon
- What must be true
- Bridging bone across the fracture plane on CT - not simply a less conspicuous line on plain films
- What must be true
- Full symmetrical elbow flexion, extension, pronation and supination compared with the other side
- What must be true
- Symmetrical triceps and forearm strength, and restored scapular, trunk and hip control - a thrower who cannot generate force through the legs and trunk generates it at the elbow
- What must be true
- A completed interval throwing programme progressing distance before intensity, then intensity before volume, then position-specific work - each stage cleared without pain the following day
- What must be true
- Throwing volume, rest intervals and mechanics reviewed, and any UCL insufficiency treated - otherwise the same load returns to the same bone
Why elite throwers are often offered fixation earlier. The argument is not that surgery heals bone better in principle, but that non-operative treatment of an established olecranon stress fracture asks a bone under repetitive tensile and impaction load to unite while the athlete waits, with an uncertain endpoint and a real risk of progression to a complete fracture or non-union - after which surgery happens anyway, later, having cost a season. Internal fixation converts an uncertain timeline into a more predictable one. The evidence underlying this is small case series rather than comparative trials, so it is a reasoned preference in a high-demand athlete rather than a proven superiority, and it should be presented to the patient as such.
Two pitfalls recur with olecranon stress fracture. First, a NORMAL plain radiograph does not exclude it: early the film is often normal, so a thrower with persistent posterior elbow pain on extension needs an MRI or CT rather than reassurance, because a missed stress fracture can progress to a complete fracture or non-union. Second, do not treat the olecranon in isolation: VALGUS INSTABILITY / UCL insufficiency loads the posteromedial elbow, drives valgus extension overload, and is a cause of recurrence, so the UCL must be assessed and addressed where indicated. Treating the bone while ignoring the ligament and the throwing load is a recipe for recurrence.
Mnemonics & Memory Aids
OLECRANON
Hook:OLECRANON: Overuse, valgus Loading, Extension pain, CT/MRI, Rest early, Adolescent vs Adult patterns, Non-union fix, Operate for elite, Note the UCL.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A baseball pitcher has posterior elbow pain worse on extension and throwing, with normal radiographs. What is your diagnosis and work-up?”
“How would you treat an olecranon stress fracture in a competitive thrower?”
Who & mechanism
- Overuse in throwing athletes (baseball/javelin) and gymnasts
- Valgus extension overload: posteromedial impingement + triceps traction
- Rising incidence with year-round youth sport
Presentation & patterns
- Posterior elbow pain worse on extension and throwing; posteromedial tenderness
- Adolescent: persistent (non-united) olecranon physis
- Adult: oblique stress fracture line
Diagnosis
- Plain films often normal early
- MRI (stress reaction/marrow oedema) or CT (line) for definitive diagnosis
- Assess valgus instability / UCL insufficiency
Management
- Rest + activity modification + graded throwing programme for early disease
- Surgical fixation (intramedullary screw or tension band; graft for non-union) for established/elite return
- Address UCL/valgus instability; modify throwing load/mechanics
Evidence & Key Studies
Olecranon Stress Fracture
- Olecranon stress fractures are a rare upper-extremity fracture that primarily affects throwing athletes, with rising incidence (especially in the paediatric population) as sport participation and volume increase.
- Their vague presentation makes diagnosis and management challenging, so careful evaluation of the disease process, diagnosis and treatment is important.
- MRI is highlighted as part of the work-up of the throwing/overuse elbow injury.
Stress reactions and fractures around the elbow in athletes
- Athletes in throwing sports and those with high repetitive/compressive loads (e.g. gymnastics) are particularly susceptible to elbow stress injuries; susceptible bones include the olecranon process (and distal humerus, coronoid, sublime tubercle, radial head).
- Diagnosis can sometimes be made on history, examination and radiography, but MRI is often required for definitive diagnosis.
- The mainstay of management is rest and activity modification, with surgical management often required for advanced pathology to achieve successful resolution and return to play.
The predominance in throwing athletes, the rising (especially paediatric) incidence and the vague presentation come from the cited Greif review; the susceptibility of throwers and high-load athletes (gymnasts), the olecranon as a susceptible site, the frequent need for MRI when radiographs are unrevealing, and the rest-mainstay-with-surgery-for-advanced-pathology approach from the cited McBride review. The valgus- extension-overload mechanism, the adolescent persistent-physis versus adult oblique-line patterns, the link to UCL/valgus instability and the specific fixation constructs (tension band / intramedullary screw) are standard, well-established teaching. The rule that the posteromedial osteophyte acts as a secondary valgus stabiliser and that resection must stop at the anatomic olecranon contour follows Valgus Extension Overload of the Elbow, so the two carry the same warning. No return-to-play interval is quoted here because the published experience is small case series rather than comparative studies, which is also why the criteria above are written as milestones to be met rather than as a timeline. (See also Elbow UCL Injury, Olecranon Fractures and Little League Elbow.)