Corns, Calluses and Intractable Plantar Keratosis
- Plantar keratoses are HYPERKERATOSES - localised thickening of the stratum corneum - produced by repetitive PRESSURE and SHEAR on the skin; the body lays down keratin to protect a focal high-load area, but the thickened skin then itself becomes a painful prominence.
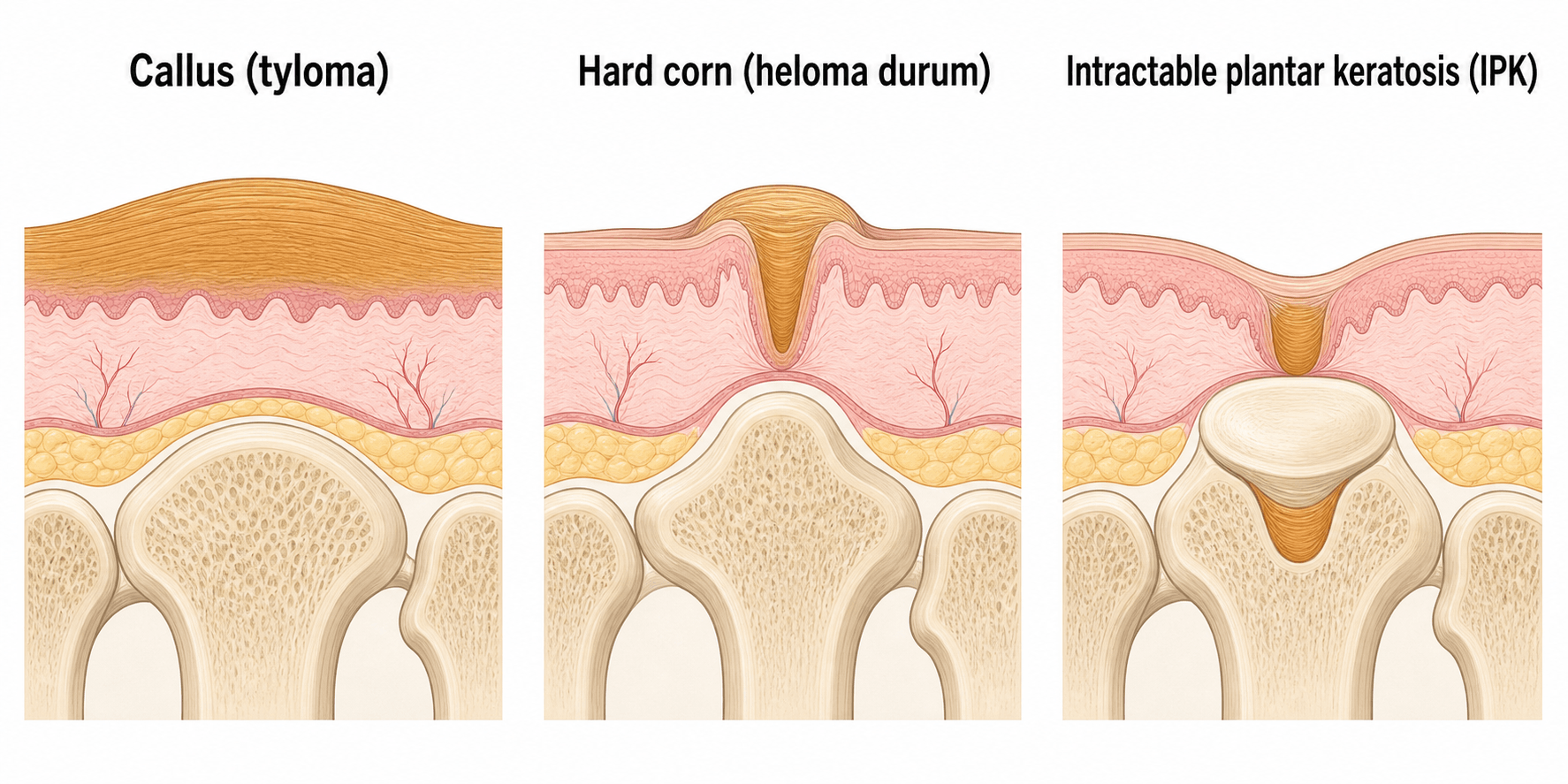
- Distinguish: a CALLUS (tyloma) is a DIFFUSE plaque over a broad weight-bearing area; a CORN (heloma) is FOCAL with a central keratin CORE - 'durum' (hard) over a bony prominence, 'molle' (soft, macerated) in a web space (classically the 4th); an INTRACTABLE PLANTAR KERATOSIS (IPK) is a discrete deep plug directly UNDER A METATARSAL HEAD.
- The cause is almost always ABNORMAL/FOCAL LOAD: a prominent or plantarflexed metatarsal head (or a prominent fibular condyle of the metatarsal head), equinus/tight gastrocnemius, claw or hammer toes, hallux valgus, pes cavus, prior surgery, or ill-fitting footwear - so treatment must address the underlying mechanics, not just the skin.
- A key exam point is differentiating an IPK from a PLANTAR WART (verruca): an IPK lies over a weight-bearing BONY point, the normal SKIN LINES (dermatoglyphics) run THROUGH it, it is tender to DIRECT pressure, and paring reveals only keratin; a VERRUCA can be anywhere, INTERRUPTS the skin lines, is tender to LATERAL pinch/squeeze, and paring reveals PINPOINT BLEEDING from thrombosed capillaries (black dots).
- In the patient with DIABETES (or neuropathy), a plantar callus is a PRE-ULCERATIVE sign - the high pressure under the callus causes underlying tissue breakdown and ulceration - so calluses must be regularly DEBRIDED and the area OFFLOADED; patients themselves often fail to notice these lesions.
- Management is CONSERVATIVE first: regular paring/debridement, padding and OFFLOADING (metatarsal dome/bar, accommodative orthoses), well-fitting/wide footwear, emollients (urea/salicylic-acid keratolytics), and correcting the cause; SURGERY is reserved for refractory IPK and aims to relieve the pressure - condylectomy (DuVries) of a prominent fibular condyle or a metatarsal OSTEOTOMY to elevate/shorten a plantarflexed metatarsal, and correction of associated toe/forefoot deformity - but carries a real risk of TRANSFER LESIONS under adjacent metatarsals.
- “Callus = diffuse (no core); corn = focal with a core (durum over bone, molle in the web); IPK = discrete plug under a met head.
- “IPK vs verruca: IPK keeps skin lines + tender to DIRECT pressure + no bleeding on paring; verruca interrupts skin lines + tender to PINCH + pinpoint bleeding.
- “Diabetic callus = pre-ulcer sign (debride + offload). Surgery for IPK relieves pressure but can cause TRANSFER lesions.
Over a weight-bearing bony point (met head). Skin lines run through it. Tender to direct pressure. Paring = keratin only, no bleeding.
Anywhere on the sole. Interrupts skin lines. Tender to lateral pinch/squeeze. Paring = pinpoint bleeding (thrombosed capillaries / black dots).
Types & Pathogenesis
Repetitive pressure and shear drive the epidermis to thicken its stratum corneum. A callus (tyloma) is the diffuse form over a broad load area; a corn (heloma) is the focal form with a central keratin core that presses inward like a nail and causes sharp pain - hard (durum) over a bony prominence (the dorsum or tip of a clawed/hammered toe, or a metatarsal head) and soft (molle), white and macerated, in a moist web space (classically the 4th) where adjacent phalangeal condyles rub. An intractable plantar keratosis (IPK) is a discrete deep plug directly under a metatarsal head, usually because that metatarsal is prominent or plantarflexed or has a prominent fibular condyle. The common thread is abnormal mechanics, so durable treatment means correcting the load.

Assessment
Examine the lesion's site and its relation to a bony prominence, the foot's deformities (claw/ hammer toes, hallux valgus, cavus, prominent/plantarflexed metatarsal, equinus), and the footwear. Pare the lesion to differentiate an IPK/callus (keratin only, preserved skin lines, tender to direct pressure) from a verruca (pinpoint bleeding, interrupted skin lines, tender to lateral pinch). Assess sensation and vascular status - critical in diabetics, where a callus is a pre-ulcer marker. Weight-bearing radiographs help identify a prominent or plantarflexed metatarsal, a long metatarsal, or a prominent fibular condyle when planning surgery.

Management
- Conservative (first line): regular paring/debridement; padding and offloading with a metatarsal dome/bar, accommodative orthoses and cushioned, wide, low-heeled footwear; emollients/keratolytics (urea, salicylic acid); and treating the underlying deformity non-operatively. For a soft corn, keep the web dry and separate the toes.
- Diabetic/neuropathic foot: regular professional debridement + offloading to prevent the callus progressing to ulceration; multidisciplinary diabetic-foot care.
- Surgery (refractory IPK / corns): aim to relieve the focal pressure -
- DuVries condylectomy: excise the prominent fibular (plantar) condyle of the metatarsal head under a discrete IPK.
- Metatarsal osteotomy (e.g. distal/BRT/Weil-type) to elevate or shorten a plantarflexed/long metatarsal.
- Correct the deformity driving a corn: hammer/claw toe correction, condylectomy of a phalangeal condyle for a soft corn, hallux valgus correction.
- Simply excising the skin lesion alone does NOT work - it recurs unless the bony cause is addressed.
Where the metatarsal pad goes - the detail that decides whether it works
An offloading pad only works if it is positioned correctly, and the commonest reason one fails is that it has been put in the wrong place.
The pad sits just PROXIMAL to the metatarsal heads, not under them. Its purpose is to support the metatarsal necks and shafts so that load is taken behind the heads and the transverse arch is lifted, which lowers the pressure at the head itself. A pad placed directly beneath the painful head does the opposite - it raises the very prominence that is causing the keratosis and makes the symptoms worse. Verify the position on the patient rather than trusting the pad's printed outline: with the pad in place, the palpable metatarsal heads should sit just distal to its leading edge.
The rest of the offloading prescription:
- A stiff or rocker sole limits dorsiflexion at the metatarsophalangeal joints and shortens the time the forefoot spends loaded at push-off - often more effective than anything placed inside the shoe.
- A wide, deep toe box for a clawed or hammered toe with a dorsal corn, so the shoe stops rubbing the prominence; a soft silicone sleeve or interdigital spacer for a soft corn, alongside keeping the web dry.
- Accommodative rather than corrective materials in the insensate foot - the aim is to spread load and cushion, not to hold a rigid correction against skin that cannot report pain.
- Full detail of the devices is in Foot & Ankle Orthotics.
Testing for the equinus you are being asked to treat
Equinus drives global forefoot overload and gastrocnemius recession is the operation that addresses it - but the contracture has to be demonstrated first, and distinguished from a tight whole triceps surae.
The Silfverskiöld test does this. Measure passive ankle dorsiflexion with the knee extended, then repeat with the knee flexed to 90 degrees, keeping the hindfoot in slight inversion so that the movement is true ankle dorsiflexion rather than midfoot break. Because gastrocnemius crosses the knee and soleus does not, flexing the knee slackens gastrocnemius alone:
- Dorsiflexion improves markedly with the knee flexed - an isolated gastrocnemius contracture, treated by a gastrocnemius recession.
- Dorsiflexion stays limited in both positions - the whole gastrocsoleus complex is tight, and a gastrocnemius recession alone will not correct it; a tendo-Achilles lengthening is the corresponding procedure, with a higher risk of over-lengthening and calcaneus gait.
The contracture and its management are developed in Gastrocnemius Equinus Contracture.
Metatarsal surgery for an IPK relieves the treated ray but commonly creates a TRANSFER LESION - a new plantar keratosis (transfer metatarsalgia) under an adjacent metatarsal head whose relative load has increased - and may precipitate a hammer-toe of the operated ray. In one long-term series of distal metatarsal osteotomies for intractable plantar callosity, although most callosities healed, new transfer callosities and hammer-toe deformities developed over time. Counsel patients accordingly, balance the rays carefully, and exhaust conservative care first - especially in low-demand or vasculopathic/diabetic patients.
Approach from the dorsum, not through the sole
Every one of these operations is reached through a dorsal incision, and the reason is worth stating plainly: a scar on weight-bearing plantar skin can be more painful and more disabling than the keratosis it was meant to cure. Plantar skin is thick and tethered by fibrous septa to the fat pad beneath it, and it takes load with every step, so an incision there heals into a firm, tender scar that becomes a focal prominence in its own right - the patient trades a callus for something that cannot be offloaded.
- Perform the condylectomy or osteotomy through a dorsal or dorsolateral incision over the relevant metatarsal or web space, working down to the plantar condyle from above.
- Do not excise the keratosis. The skin is the symptom; removing it leaves a wound in a high-pressure area and the lesion returns unchanged once the bone beneath it is untouched.
- If a plantar incision is genuinely unavoidable, place it longitudinally and away from the loaded metatarsal heads and heel, in the relatively unloaded arch.
- The same logic is sharper in the diabetic foot, where a plantar wound in an insensate, poorly perfused ray is how an elective procedure becomes an ulcer.
The Metatarsal Parabola: Why One Ray Overloads (and Transfer Lesions)
- Normal forefoot load is a harmonious cascade: the metatarsal heads share weight in a smooth "parabola" - the second metatarsal is usually the longest, with the others progressively shorter from the second to the fifth, and the first ray (with its sesamoids) carries its share. Load is distributed across all the heads.
- Why one ray overloads: a metatarsal that is relatively long, plantarflexed, or carries a prominent plantar (fibular) condyle bears excess focal pressure → an IPK forms under it; and an insufficient or hypermobile first ray (e.g. hallux valgus or a failed bunion operation) shifts load laterally to the second/third heads, while equinus raises global forefoot pressure.
- The surgical corollary and the transfer-lesion mechanism: osteotomy aims to restore the harmonious parabola by shortening/elevating the offending metatarsal - but over-correcting or unbalancing the cascade shifts the relative load to an adjacent head, producing a new IPK (transfer lesion). This is why the rays must be balanced, why transfer lesions are common (the cited series), and why focal skin excision alone fails. (General forefoot overload is in Metatarsalgia.)
The forefoot bears load as a parabola (2nd metatarsal usually longest, then progressively shorter to the 5th). A long/plantarflexed metatarsal or prominent fibular condyle overloads one head → IPK; an insufficient first ray transfers load laterally. Surgery restores the cascade - but unbalancing it moves the lesion to the next head (transfer lesion), so balance the rays and don't just excise skin.
Discrete vs Diffuse IPK (and the Porokeratosis Mimic)
- Discrete (localised) IPK: a single, well-defined plug under one metatarsal head, classically over a prominent plantar (fibular) condyle - addressed by removing that focal prominence (DuVries condylectomy) or a focal elevating osteotomy.
- Diffuse IPK: a broader keratosis under several (often the central) metatarsal heads, reflecting a global forefoot overload - a long/plantarflexed metatarsal cascade, equinus/tight gastrocnemius, pes cavus, or first-ray insufficiency - so treatment addresses the global cause (e.g. gastrocnemius recession for equinus, rebalancing the cascade, cavus correction) rather than a single condylectomy.
- The look-alike - porokeratosis plantaris discreta: a deep, sharply-demarcated, very tender keratotic plug arising from a sweat (eccrine) duct, not over a bony prominence and pressure-independent - it mimics an IPK, and recognising it avoids a futile metatarsal osteotomy (excise/treat the lesion itself).
Separate discrete IPK (one head, over a prominent fibular condyle → condylectomy/focal osteotomy) from diffuse IPK (several heads, a global problem - long cascade, equinus, cavus, first-ray insufficiency → treat the global cause, e.g. gastrocnemius recession). Beware porokeratosis plantaris discreta - a sweat-duct plug not over bone and pressure-independent - which mimics an IPK but won't respond to a metatarsal osteotomy.
Mnemonics & Memory Aids
LINES
Hook:Skin LINES through it + direct-pressure pain + no bleeding = IPK, not a verruca.
PADS
Hook:Treat with PADS - offload first, surgery (with transfer-lesion caution) last.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a painful discrete callus under the second metatarsal head. How do you confirm it is not a wart, and how would you manage it?”
“Why does a plantar callus matter more in a patient with diabetes, and how does that change your management?”
Definitions
- Callus (tyloma): diffuse, no core
- Corn (heloma): focal + central core - durum (over bone), molle (web space, macerated)
- IPK: discrete deep plug under a metatarsal head
IPK vs verruca
- IPK: over bony point, skin lines THROUGH it, tender to DIRECT pressure, keratin only
- Verruca: anywhere, INTERRUPTS skin lines, tender to PINCH, pinpoint bleeding on paring
- Pare the lesion to differentiate
Cause & diabetic significance
- Abnormal load: prominent/plantarflexed metatarsal, fibular condyle, claw/hammer toes, cavus, equinus, footwear
- Diabetic callus = PRE-ULCER sign (debride + offload)
- Patients under-recognise their own calluses
Management
- Conservative: pare/debride, offload (met dome/orthoses), footwear, keratolytics, treat deformity
- Soft corn: keep web dry + separate toes
- Surgery (refractory): DuVries condylectomy / metatarsal osteotomy -> beware transfer lesions
Evidence & Key Studies
Straight (transverse distal) metatarsal osteotomy for the treatment of plantar callosities
- In 25 intractable plantar callosities treated by transverse distal metatarsal osteotomy, 23 had healed at 7-year follow-up (two after re-osteotomy).
- However, eight hammer-toe deformities developed in operated rays and eight new plantar callosities developed under adjacent (non-operated) rays - i.e. transfer lesions.
- Metatarsal osteotomy is effective for intractable plantar callosity but transfer lesions and hammer toes tend to develop over time - a key counselling point.
Differences between patient-reported and clinician-observed nonulcerative foot signs in diabetes
- Calluses and corns are recognised non-ulcerative (pre-ulcerative) foot signs in patients with diabetes at risk of foot ulceration.
- Patients poorly self-identified these lesions (sensitivity ~51% for calluses and ~44% for corns), so many high-pressure lesions go unnoticed by the patient.
- Supports professional surveillance, debridement and patient education/offloading to reduce diabetic foot ulcer risk.
The efficacy of metatarsal osteotomy for IPK and the development of transfer lesions/ hammer toes come from the cited Kiviniemi series, and the pre-ulcerative significance of calluses/corns in diabetes (and patients' poor self-recognition) from the cited Takehara study. The corn/callus/IPK definitions and the IPK-versus-verruca differentiation are standard clinical teaching, as are the metatarsal-pad position, the Silfverskiold test and the dorsal-approach principle. (See also Metatarsalgia, Lesser Toe Deformities, Claw Toes, Diabetic Foot, Gastrocnemius Equinus Contracture and Foot & Ankle Orthotics.)