First MTP Joint Decompression
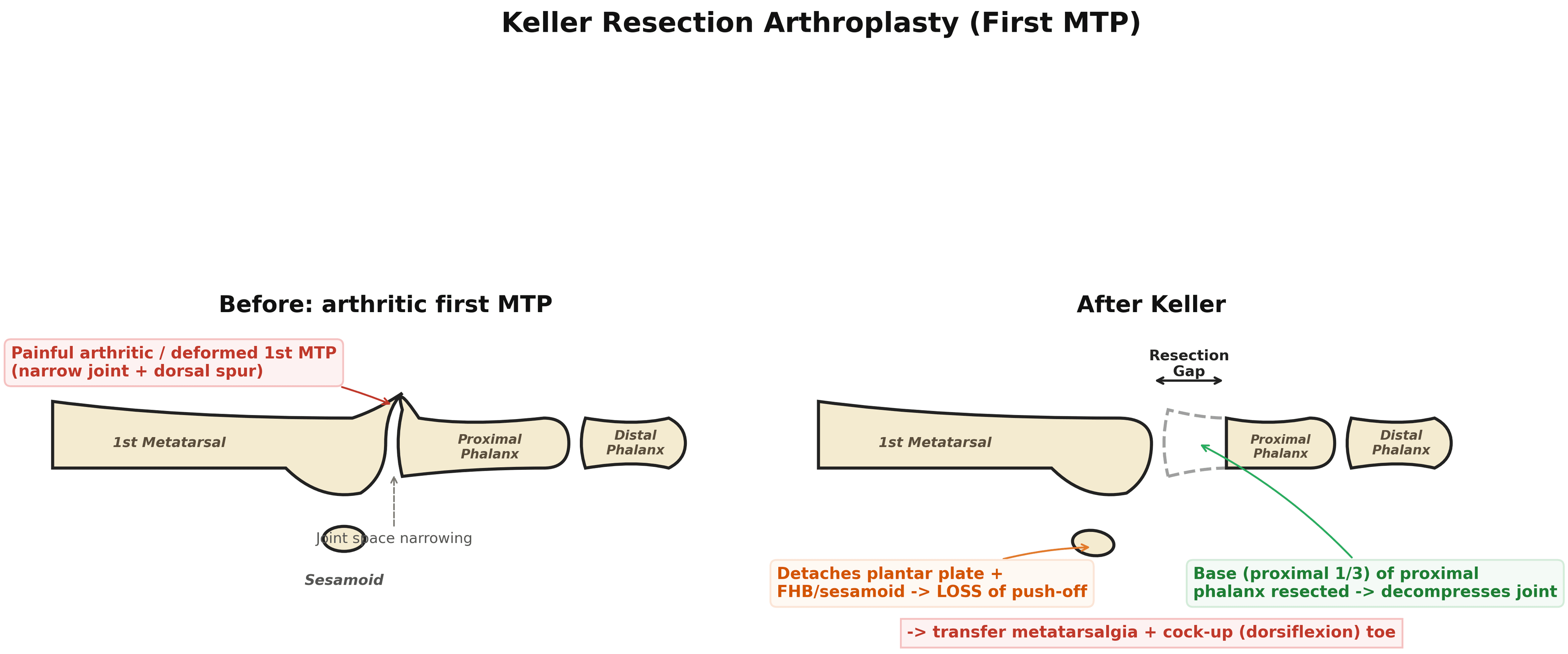
- The Keller procedure is a RESECTION ARTHROPLASTY of the first metatarsophalangeal joint, performed by excising the BASE (the proximal third) of the PROXIMAL PHALANX of the hallux; this decompresses the arthritic or deformed first MTP joint, relieving pain and improving the alignment of a bunion (radiographs show a reduced intermetatarsal and first-MTP angle in many cases).
- Its INDICATIONS have narrowed over time: although historically used widely for hallux valgus and hallux rigidus, the Keller is now reserved largely for the LOW-DEMAND, ELDERLY patient with a painful arthritic and/or deformed first MTP joint (and sometimes for ulcerated/at-risk first MTP joints), and as a salvage option - it is generally avoided in young, active or high-demand patients.
- The fundamental TRADE-OFF is loss of HALLUX FUNCTION: resecting the base of the proximal phalanx detaches the plantar plate and the intrinsic (flexor hallucis brevis/sesamoid) mechanism and disrupts the windlass mechanism, so the hallux loses its PUSH-OFF and weight-bearing role, transferring load to the lesser metatarsals.
- The characteristic COMPLICATIONS follow from that trade-off: TRANSFER METATARSALGIA (pain under the lesser metatarsal heads from load transfer), a COCK-UP (dorsiflexion/hyperextension) deformity of the hallux, a flail, floppy or excessively short toe, recurrent valgus deformity, and cosmetic shortening - and although complications are common, in elderly low-demand patients pain relief and footwear tolerance are often still satisfactory.
- Because of these drawbacks, the Keller has been LARGELY SUPERSEDED for hallux valgus by corrective bunion OSTEOTOMIES and for hallux rigidus by CHEILECTOMY (early grades) and first MTP ARTHRODESIS (advanced disease, especially in active patients) - so the modern role of the Keller is the limited niche of the low-demand elderly patient.
- When a Keller FAILS - typically with recurrent valgus, a cock-up deformity, a flail toe or transfer metatarsalgia - the recommended SALVAGE is FIRST MTP ARTHRODESIS, which gives higher patient satisfaction and better clinical results than a repeat Keller or an isolated soft-tissue release (though it is technically demanding because of the bone loss and may need bone grafting to restore length).
- “Keller = resection arthroplasty of the first MTP - excise the BASE (proximal third) of the proximal phalanx of the hallux to decompress the joint.
- “Modern niche: LOW-DEMAND ELDERLY with hallux valgus / hallux rigidus (avoid in active/high-demand). Loses hallux push-off -> TRANSFER METATARSALGIA, COCK-UP deformity, flail/short toe, recurrent valgus.
- “Largely superseded by bunion osteotomies (HV) and cheilectomy/arthrodesis (hallux rigidus). Salvage of a failed Keller = first MTP ARTHRODESIS (better than repeat Keller).
Excise the base of the proximal phalanx to decompress the first MTP - now reserved for the low-demand elderly with hallux valgus/hallux rigidus (avoid in the active).
Loses hallux push-off -> transfer metatarsalgia, cock-up deformity, flail/short toe, recurrence. Failed Keller -> first MTP arthrodesis (salvage).
Procedure, Indication & Trade-off
The Keller procedure is a resection arthroplasty of the first MTP joint - excising the base (proximal third) of the proximal phalanx of the hallux to decompress an arthritic/deformed joint, relieving pain and improving bunion alignment. Its modern niche is the low-demand, elderly patient with a painful arthritic and/or deformed first MTP (hallux valgus or hallux rigidus), and as a salvage - it is generally avoided in active/high-demand patients. The trade-off is loss of hallux push-off: resecting the phalangeal base detaches the plantar plate and the intrinsic (flexor hallucis brevis/sesamoid) mechanism and disrupts the windlass, so load transfers to the lesser metatarsals. Hence the complications - transfer metatarsalgia, a cock-up (dorsiflexion) deformity, a flail/floppy/short toe, and recurrent valgus. It has been largely superseded by bunion osteotomies and by cheilectomy/arthrodesis for hallux rigidus, and a failed Keller is salvaged by first MTP arthrodesis.
- Mechanism
- Excise base of proximal phalanx (decompress)
- Best for
- Low-demand elderly (HV / hallux rigidus); salvage
- Mechanism
- Remove dorsal osteophyte/spur (preserve joint)
- Best for
- Early hallux rigidus (grade 1-2)
- Mechanism
- Fuse the joint
- Best for
- Advanced hallux rigidus / active patients; failed Keller salvage
- Mechanism
- Realign the metatarsal/phalanx
- Best for
- Hallux valgus (active patients)
Complications & Salvage
- Transfer metatarsalgia: loss of hallux weight-bearing transfers load to the lesser metatarsal heads - the commonest functional complaint.
- Cock-up (dorsiflexion) deformity of the hallux, and a flail/floppy or excessively short toe (from detachment of the intrinsics/plantar plate and over-resection).
- Recurrent valgus deformity and cosmetic shortening.
- Avoid in the active/high-demand patient (push-off loss is poorly tolerated); reserve for the low-demand elderly.
- Salvage of a failed Keller = first MTP arthrodesis (better satisfaction/results than a repeat Keller or soft-tissue release), often with bone graft to restore length - technically demanding because of the bone loss.
The Keller resection arthroplasty survives in modern practice only as a limited-niche operation, and the two errors to avoid are using it in the wrong patient and mismanaging its failures. Because resecting the base of the proximal phalanx destroys the hallux's push-off and weight-bearing role, it should NOT be offered to a young, active or high-demand patient - in whom it predictably causes transfer metatarsalgia and a weak, cock-up toe - and is instead reserved for the low-demand elderly patient with a painful arthritic or deformed first MTP, where pain relief and footwear tolerance are usually satisfactory despite the complications. When a Keller fails, with recurrent valgus, a cock-up deformity, a flail toe or transfer metatarsalgia, the reliable salvage is a first MTP arthrodesis rather than a repeat Keller; it is more technically demanding because of the bone loss and may need bone grafting, but it gives far better satisfaction. In active patients, bunion osteotomies (for hallux valgus) and cheilectomy or arthrodesis (for hallux rigidus) are the appropriate alternatives.
The Diabetic Hallux Ulcer: Where the Keller Is Still First Choice
Beyond the low-demand elderly bunion, the Keller has a second and arguably more active modern role, in which the very feature that limits it elsewhere becomes the point of the operation.
A neuropathic plantar ulcer under the hallux or the first metatarsal head is driven by peak pressure at push-off in a foot with a stiff, arthritic or clawed first MTP. Offloading devices work, but require the patient to comply indefinitely. Resecting the base of the proximal phalanx decompresses the joint, restores dorsiflexion and drops the peak plantar pressure under the first ray - a permanent, structural offloading that does not depend on the patient wearing anything. This is often called surgical offloading, and the Keller sits alongside flexor tenotomy and metatarsal osteotomy in that group.
The considerations specific to this use:
- Vascular status first. A neuropathic ulcer in an ischaemic foot needs revascularisation before, or instead of, any elective bone resection - the wound will not heal on a poorly perfused ray whatever is done to the joint.
- Infection must be assessed. An ulcer probing to bone means osteomyelitis until proven otherwise, and changes the operation from an elective offloading procedure to a debridement with bone resection and culture-directed antibiotics.
- The loss of push-off is not the problem it is elsewhere. These patients are typically low-demand, already have an insensate foot and a disturbed gait, and the trade of push-off for a healed ulcer is usually the right one.
- Transfer is still the risk. Offloading the first ray predictably shifts load laterally, so warn about, and monitor for, a transfer ulcer under the lesser metatarsal heads - the ulcer equivalent of transfer metatarsalgia.
The broader ulcer pathway, including non-surgical offloading, belongs to Diabetic Foot Ulcers and Foot & Ankle Orthotics.
First-Ray Biomechanics: Why Resecting the Base Costs Push-Off
- The first ray is the main push-off lever. The hallux and first MTP transmit a large share of forefoot load at terminal stance/toe-off; a competent first ray is needed to drive push-off.
- The windlass (Hicks) mechanism: in terminal stance, dorsiflexion of the hallux winds the plantar aponeurosis around the metatarsal head, shortening it, raising the medial arch and locking the midfoot into a rigid lever for push-off.
- The sesamoid-FHB complex: the two sesamoids sit within the medial and lateral heads of flexor hallucis brevis (with abductor/adductor hallucis), glide under the metatarsal head, bear load and cushion it, and increase the FHB plantarflexion moment arm. This plantar plate / FHB / sesamoid sling inserts onto the BASE of the proximal phalanx.
- So resecting the base detaches the whole sling: active hallux plantarflexion and the windlass are abolished, the hallux no longer purchases the ground or stiffens the foot, and load transfers to the lesser metatarsal heads (transfer metatarsalgia). With the intrinsic flexor anchor gone, the unopposed long extensor pulls the toe into the cock-up (dorsiflexion) deformity, and the shortened, destabilised toe becomes flail. (Sesamoid and plantar-plate pathology in their own right are covered in Sesamoid Disorders and Plantar Plate Insufficiency.)
The plantar plate / FHB / sesamoid sling and the windlass anchor on the base of the proximal phalanx - the exact bone the Keller removes. That single fact explains the whole complication list: no windlass/push-off → transfer metatarsalgia; lost intrinsic flexor anchor with unopposed extensor → cock-up; shortening + destabilisation → flail/short toe.
Doing the Keller Well: Technique That Limits the Complications
Several operative principles are taught to limit the complications, each following from the biomechanics above:
- Approach: a dorsomedial (or medial) longitudinal incision over the first MTP; protect the dorsomedial cutaneous nerve; excise the medial eminence if there is a bunion.
- Resect conservatively - only the proximal third: removing about a third of the proximal phalanx decompresses the joint while preserving length; over-resection gives a flail/short/floppy toe, while under-resection leaves inadequate decompression, stiffness and recurrence.
- Preserve and reattach the soft tissues: where possible reattach the plantar plate / flexor hallucis
brevis to the residual phalangeal base or capsule and interpose capsule/soft tissue over the cut surface
- this retains some active plantarflexion and resists the cock-up deformity.
- Hold length and alignment: a temporary longitudinal K-wire across the MTP keeps the toe out to length in slight plantarflexion and correct rotation while the soft tissues scar in, reducing cock-up and excessive shortening; remove it after a few weeks.
- Rehabilitation: a stiff-soled/heel-weight-bearing shoe and early mobilisation. (The salvage fusion technique is developed in First MTP Arthrodesis.)
Technique that limits failure: resect only the proximal third (over-resection → flail/short toe; under-resection → recurrence), reattach the plantar plate/FHB and interpose capsule, and hold the toe out to length on a temporary K-wire in slight plantarflexion for a few weeks - then early mobilise. Doing this mitigates the cock-up deformity and shortening.
How much of this is actually proven?
These principles are mechanically coherent, and they are what is taught - but be careful about asserting them as established fact, because the clinical evidence is thinner than the reasoning. In the 49-foot series cited below, the amount of proximal phalanx resected showed no association with either metatarsalgia or the final outcome, and, more surprisingly, the occurrence of complications showed no association with the final result or the patient's functional grade either.
Two honest conclusions follow. The biomechanical case for conservative resection stands - detaching the flexor sling is what produces the cock-up toe, and taking less bone leaves more to reattach to - so resect a third rather than a half. But the claim that outcome tracks resection length is unsupported, and in a low-demand elderly patient a radiographically imperfect result with a documented complication frequently still gives a satisfied patient in comfortable shoes. That mismatch between anatomical result and reported satisfaction is precisely why the operation persists in this narrow group, and why it should not be judged by the standards applied to a fusion in an active patient.
Mnemonics & Memory Aids
KELLER
Hook:KELLER: Knock off the phalangeal base, Elderly low-demand niche, Loses push-off, Lesser-MTP transfer metatarsalgia, Erect (cock-up) toe, Rescue with arthrodesis.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is the Keller procedure and what is its modern role?”
“How would you salvage a failed Keller arthroplasty?”
Procedure
- Resection arthroplasty of the first MTP joint
- Excise the base (proximal third) of the proximal phalanx of the hallux
- Decompresses the joint; reduces IM/MTP angles in many cases
Indication (modern)
- Low-demand elderly with painful arthritic/deformed first MTP (HV / hallux rigidus)
- Salvage option
- Avoid in young/active/high-demand patients
Complications
- Transfer metatarsalgia (lost push-off -> lesser-MTP overload)
- Cock-up (dorsiflexion) deformity; flail/floppy/short toe
- Recurrent valgus; cosmetic shortening
Alternatives & salvage
- Cheilectomy (early hallux rigidus); first MTP arthrodesis (advanced/active); bunion osteotomy (HV)
- Failed Keller -> first MTP arthrodesis (better than repeat Keller)
- Often needs bone graft to restore length at salvage
Evidence & Key Studies
Keller's arthroplasty in adults with hallux valgus and hallux rigidus
- In 32 patients (49 feet, mean age 62.5 years) with hallux valgus and hallux rigidus, Keller's resection arthroplasty gave satisfactory pain relief, cosmesis and footwear use, with excellent/good results in 87% by the Bonney-MacNab criteria.
- Radiographs showed a decrease in the intermetatarsal and first metatarsophalangeal angles in many cases.
- Complications were common but were not associated with the final result, and the amount of phalangeal-base resection was not associated with metatarsalgia or outcome.
Salvage of a failed Keller resection arthroplasty (arthrodesis vs motion-preserving)
- Typical complications of the Keller procedure include recurrent valgus deformity, cock-up deformity and a flail toe.
- First metatarsophalangeal arthrodesis as salvage achieved fusion in 26 of 29 feet with excellent/good satisfaction in 23, whereas a repeat Keller or isolated soft-tissue release gave excellent/good results in only 6 of 21 (with recurrent valgus/cock-up in most).
- Arthrodesis is recommended for salvage of a failed Keller because of its higher satisfaction and better clinical results.
The satisfactory pain/cosmesis/footwear outcomes of Keller's arthroplasty in elderly adults with hallux valgus and hallux rigidus (with reduced IM/MTP angles, and complications not predicting the result) come from the cited Putti series; the typical complications (recurrent valgus, cock-up deformity, flail toe) and the superiority of first MTP arthrodesis over a repeat Keller/soft-tissue release for salvage from the cited Machacek study. The mechanism (resection of the proximal phalangeal base disrupting push-off, causing transfer metatarsalgia), the modern restriction to low-demand elderly patients, the surgical-offloading role in the neuropathic hallux ulcer, and the alternatives (cheilectomy, arthrodesis, bunion osteotomy) are standard, well-established teaching. The finding that neither the amount of phalangeal resection nor the occurrence of complications was associated with the final outcome also comes from the cited Putti series - a 49-foot retrospective review, so a signal rather than a settled fact. (See also Hallux Rigidus, Hallux Valgus, First MTP Arthrodesis and Metatarsalgia.)