Physiological C2-C3 Displacement in Children
- Pseudosubluxation is a PHYSIOLOGICAL (normal) anterior displacement of C2 on C3 (and sometimes C3 on C4) of up to about 2-3 mm seen in young children - it is a NORMAL VARIANT and NOT an injury, and it occurs because the immature cervical spine has ligamentous laxity, relatively horizontal facet joints, and a high fulcrum of flexion-extension motion (around C2-C3) together with a large head-to-body ratio.
- It is common and age-related: C2-C3 pseudosubluxation has been reported in around 9% of children younger than 7 years, and it generally resolves as the spine matures; it is the single most important paediatric cervical normal variant to recognise so as not to misdiagnose a normal child as having a fracture-dislocation.
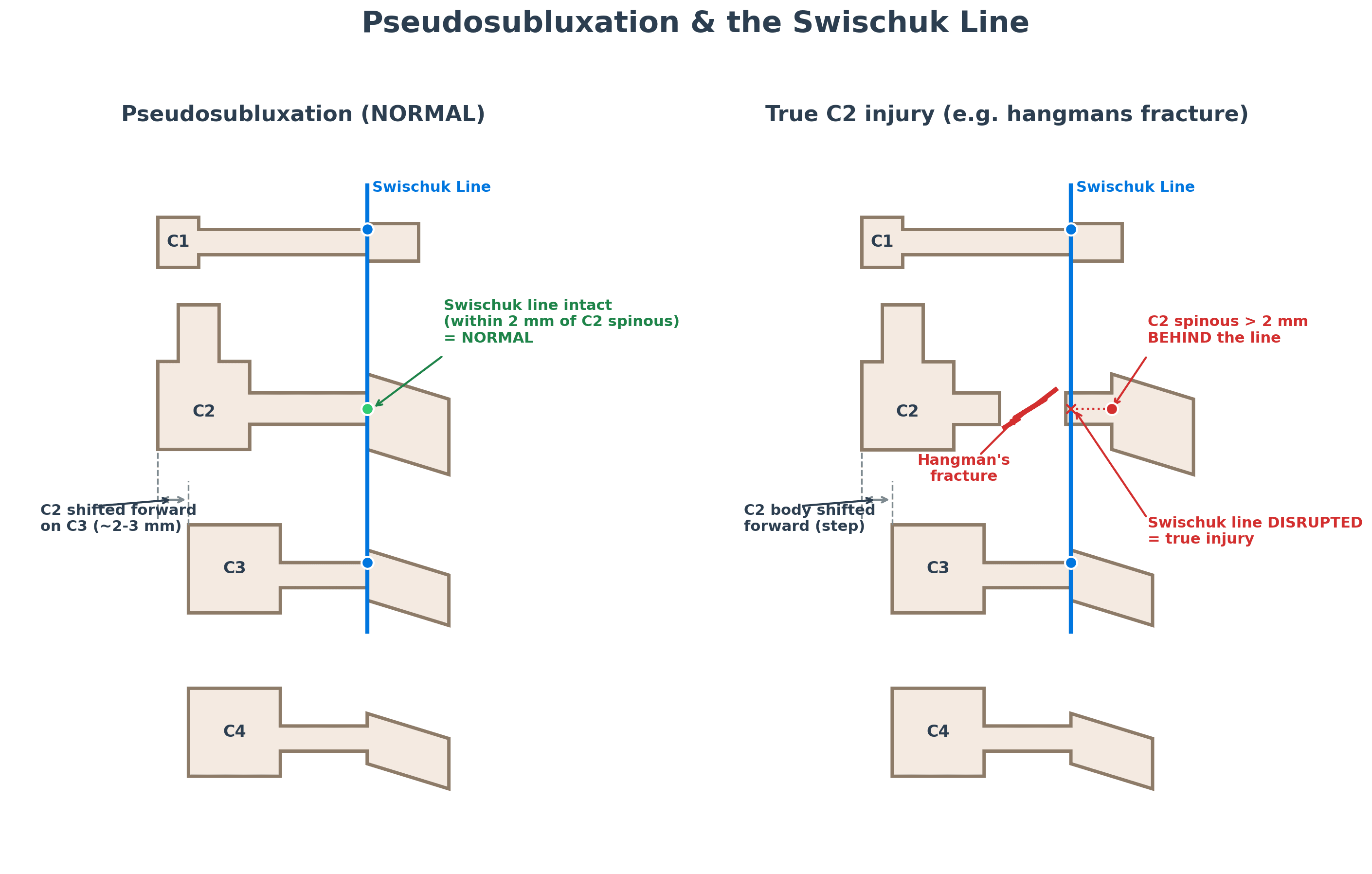
- The key tool to distinguish pseudosubluxation from a true injury is the SWISCHUK POSTERIOR CERVICAL (spinolaminar) LINE. Draw it between the anterior cortex of the C1 spinous process and the anterior cortex of the C3 spinous process - C1 TO C3 ONLY - then judge C2 against it. Drawing the line THROUGH C2 is the commonest error and destroys the test, because a line through a point always passes through it. In physiological pseudosubluxation the anterior cortex of the C2 spinous process lies within about 2 mm of the C1-C3 line; in a true C2 injury such as a hangman's fracture the posterior arch of C2 stays with C3 while the body displaces forward, so C2 falls more than 2 mm BEHIND the line.
- Further reassuring features are that pseudosubluxation REDUCES on an EXTENSION (or neutral) view, the alignment is smooth without a focal kyphotic angulation, there is no prevertebral soft-tissue swelling beyond the normal range, and there is no fracture - so correlating the radiograph with the child's AGE, the MECHANISM of injury and the clinical examination is essential.
- Pseudosubluxation sits among a family of paediatric cervical NORMAL VARIANTS that can each be mistaken for trauma: hypermobility and pseudospread of the atlas on the axis, absence of the normal cervical lordosis, anterior WEDGING of the (still partly cartilaginous) vertebral bodies, prevertebral soft-tissue PSEUDOWIDENING (worse on expiration/neck flexion), and incomplete ossification with open synchondroses - knowing these prevents over-diagnosis.
- The practical consequence is to AVOID OVER-TREATING a normal variant: recognise physiological pseudosubluxation with the Swischuk line and clinical correlation rather than immobilising or investigating a normal child unnecessarily - while still remembering that children (especially under 8) are prone to upper cervical injuries and SCIWORA, so genuine clinical concern warrants appropriate assessment.
- “Pseudosubluxation = NORMAL anterior displacement of C2 on C3 (and C3 on C4) up to ~2-3 mm in young children (~9% under age 7) - a variant, not an injury.
- “Use the SWISCHUK posterior cervical line: within ~2 mm of the C2 spinolaminar cortex = normal; disrupted = true C2 injury. It reduces on extension.
- “Other paediatric variants mimic trauma (pseudospread, anterior wedging, prevertebral pseudowidening); correlate with age/mechanism - don't over-treat.
Anterior displacement of C2 on C3 (up to ~2-3 mm) in a young child - a normal variant from laxity, horizontal facets and a high motion fulcrum.
The Swischuk posterior cervical line is intact (within ~2 mm of the C2 spinolaminar cortex), and it reduces on extension. Correlate with age/mechanism.
What It Is & How to Tell It From Injury
Pseudosubluxation is the physiological anterior displacement of C2 on C3 (and sometimes C3 on C4) of up to about 2-3 mm in young children - a normal variant, not an injury - caused by ligamentous laxity, horizontal facet joints and a high (C2-C3) fulcrum of motion with a large head-to-body ratio. It is common, reported in around 9% of children under 7, and resolves with maturity. The key way to confirm it is normal is the Swischuk posterior cervical (spinolaminar) line: drawn between the anterior cortex of the C1 and C3 spinous processes - not through C2 - with the anterior cortex of the C2 spinous process then judged against it. It should lie within about 2 mm of that line in pseudosubluxation, and more than 2 mm behind it in a true C2 injury such as a hangman's fracture. Pseudosubluxation also reduces on extension, has smooth alignment, and shows no fracture or abnormal prevertebral swelling.
Other Variants & Practical Approach
- Know the family of normal variants. Besides pseudosubluxation: hypermobility and pseudospread of the atlas on the axis, absence of lordosis, anterior wedging of the partly-cartilaginous vertebral bodies, prevertebral soft-tissue pseudowidening (worse on expiration/flexion), and incomplete ossification/open synchondroses.
- Use the Swischuk line and an extension view. An intact posterior cervical line and reduction on extension confirm a normal variant.
- Correlate with age, mechanism and examination. Interpret the paediatric cervical radiograph in light of the child's age, the injury mechanism and the clinical picture - not in isolation.
- Don't over-treat - but don't be complacent. Avoid unnecessary immobilisation/investigation of a normal variant, while remembering young children are prone to upper cervical injuries and SCIWORA, so genuine clinical concern still warrants proper assessment (and advanced imaging where indicated).
The single most useful skill with paediatric pseudosubluxation is using the Swischuk posterior cervical line to separate a normal variant from a true injury: draw the line between the spinolaminar cortices of C1 and C3 - never through C2 - and if the C2 spinous process lies within about 2 mm of it and the displacement reduces on extension, the C2-on-C3 'subluxation' is physiological; if C2 sits more than 2 mm behind the line, suspect a true C2 injury such as a hangman's fracture. Equally important is the converse caution - children under 8 are prone to upper cervical injuries and to SCIWORA (spinal cord injury without radiographic abnormality), so a normal-looking radiograph does not exclude injury when there is real clinical concern, and the radiograph must always be read with the child's age, mechanism and examination in mind.
The Normal Paediatric Measurements (Don't Over-call)
Over-calling prevertebral swelling and pseudospread is avoided by knowing the values, and the paediatric normal ranges differ from the adult (instability thresholds are developed in Atlantoaxial Instability).
- Atlanto-dental interval (ADI). The gap between the anterior arch of C1 and the dens is normally wider in children - up to about 5 mm (versus around 3 mm in adults) because of greater ligamentous laxity; a value beyond this suggests atlantoaxial instability / transverse-ligament insufficiency.
- Prevertebral soft tissue. Narrow above the larynx and wider below; a working rule is up to about 7 mm at C2 (roughly two-thirds of a vertebral-body width) and up to about 14 mm at C6 in a child. Note that the C6 figure is the paediatric one - the adult upper limit is around 21 mm, so applying the adult number to a child under-calls a genuine haematoma. It is markedly exaggerated on expiration, neck flexion or crying (pseudowidening) - so obtain a neutral inspiratory film before calling it a haematoma.
- Pseudospread of the atlas (Jackson). The C1 lateral masses can overhang the C2 body by a few millimetres in young children because the ossification centres of C1 and C2 grow at different rates - so the adult "combined lateral overhang implies a Jefferson burst fracture" rule does not apply in the young child.
Know the paediatric numbers: ADI up to about 5 mm is normal in a child (vs ~3 mm adult); prevertebral soft tissue up to roughly 7 mm at C2 / 14 mm at C6, and pseudowidening worsens on expiration/flexion - repeat neutral and inspiratory. Pseudospread (C1 overhanging C2) is normal from differential ossification, so do not call it a Jefferson fracture in a young child.
Developmental Ossification: the Synchondroses That Mimic Fractures
Incomplete ossification, open synchondroses, differential ossification-centre growth and partly-cartilaginous bodies all stem from the same developmental anatomy - and the open synchondroses are the classic fracture mimics (the odontoid in detail is in Odontoid Fractures).
- The axis (C2). Forms from several centres - the body, two neural arches and the dens (from paired centres) with an apical ossiculum terminale. The dentocentral (subdental/basilar) synchondrosis between the dens and body is a smooth corticated lucency that fuses around 3-6 years and is the classic dens-fracture mimic in young children; the ossiculum terminale appears about 3-6 years and fuses by about 12; the neurocentral synchondroses (body-to-arch) fuse around 3-6 years.
- The atlas (C1). Three centres (the anterior arch and two posterior/neural arches); the anterior arch is often unossified at birth (ossifying about a year) and the posterior synchondrosis fuses around 3-4 years.
- Telling a synchondrosis from a fracture. A synchondrosis is smooth, corticated (sclerotic margins), symmetric and at a typical anatomical site; a fracture is irregular, non-corticated, asymmetric and not at a synchondrosis line. The normally partly-cartilaginous, anteriorly-wedged vertebral bodies likewise explain the anterior-wedging variant.
The fracture mimics are synchondroses: the dentocentral synchondrosis (dens-body, fuses ~3-6 y) looks like a dens fracture, and unfused C1/C2 arch synchondroses look like arch fractures. Distinguish them - a synchondrosis is smooth, corticated, symmetric, at a typical site; a fracture is irregular, non-corticated, asymmetric, off-site. Differential ossification-centre growth also explains pseudospread and anterior wedging.
Mnemonics & Memory Aids
SWISCHUK
Hook:SWISCHUK: the line Within ~2 mm, Intact/smooth, Subluxation reduces on extension, C2-C3, Horizontal facets, Under 8, Keep clinical context (SCIWORA).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A young child's lateral cervical radiograph after a fall shows anterior displacement of C2 on C3. How do you decide if this is a normal variant or an injury?”
“What other paediatric cervical radiographic variants can mimic trauma?”
What it is
- Physiological anterior displacement of C2 on C3 (+/- C3 on C4) up to ~2-3 mm
- Normal variant in young children (~9% under age 7); resolves with maturity
- Cause: ligamentous laxity, horizontal facets, high motion fulcrum, big head
Confirm it's normal
- Swischuk posterior cervical line within ~2 mm of the C2 spinolaminar cortex
- Reduces on extension; smooth alignment; no fracture
- No abnormal prevertebral soft-tissue swelling
Other variants
- Pseudospread of atlas on axis; absence of lordosis
- Anterior wedging of vertebral bodies; prevertebral pseudowidening
- Incomplete ossification / open synchondroses
Practical approach
- Correlate with age, mechanism and examination
- Don't over-treat a normal variant
- Remember upper-cervical injuries and SCIWORA in the young
Evidence & Key Studies
Pediatric cervical spine in emergency: normal anatomy, variants and pitfalls
- The paediatric cervical spine has distinct radiographic features - hypermobility between C2 and C3, pseudospread of the atlas on the axis, pseudosubluxation, absence of lordosis, anterior wedging of vertebral bodies, prevertebral soft-tissue pseudowidening and incomplete ossification/synchondroses - that can be mistaken for traumatic injuries.
- Younger children (under 8 years) tend to sustain upper cervical injuries because of the anatomy and biomechanics of the immature spine.
- Interpretation must take into account the child's age, the location of any injury and the mechanism of trauma; comprehensive knowledge of normal variants prevents over-diagnosis.
Acute evaluation and management of pediatric spinal cord injury (C2-C3 pseudosubluxation)
- Radiographic evaluation of the child's cervical spine is challenging because of normal variants such as C2-C3 pseudosubluxation, which occurs in about 9% of children younger than 7 years.
- SCIWORA (spinal cord injury without radiographic abnormality) is common in children under 10 and is associated with more complete neurological injuries.
- Children cannot be evaluated and treated as small adults; immobilisation and imaging must account for the larger head-to-torso ratio and the upper-cervical injury pattern.
The catalogue of paediatric cervical normal variants that mimic trauma (pseudosubluxation, pseudospread, anterior wedging, prevertebral pseudowidening, incomplete ossification) and the principle of correlating with age/location/mechanism come from the cited Adib review; the prevalence of C2-C3 pseudosubluxation (about 9% under age 7) and the importance of SCIWORA in young children from the cited Betz review. The Swischuk posterior cervical line and the reduction on extension are standard, well-established teaching, as is drawing the line from C1 to C3 rather than through C2. The paediatric atlanto-dens interval of up to 5 mm follows Atlantoaxial Instability, so the two pages carry the same threshold; note that the prevertebral figure quoted here at C6 is the paediatric one and differs deliberately from the adult value used in the general spine-imaging topic. (See also SCIWORA, Hangman's Fracture, Odontoid Fractures and Systematic Spine Imaging.)