When the Sixth-Compartment Tendon Leaves Its Groove
- The extensor carpi ulnaris (ECU) runs in the SIXTH dorsal compartment within its OWN fibro-osseous SUBSHEATH, in a bony GROOVE on the dorsal aspect of the ulnar head; this subsheath (distinct from the overlying extensor retinaculum) is what keeps the ECU in its groove during forearm rotation.
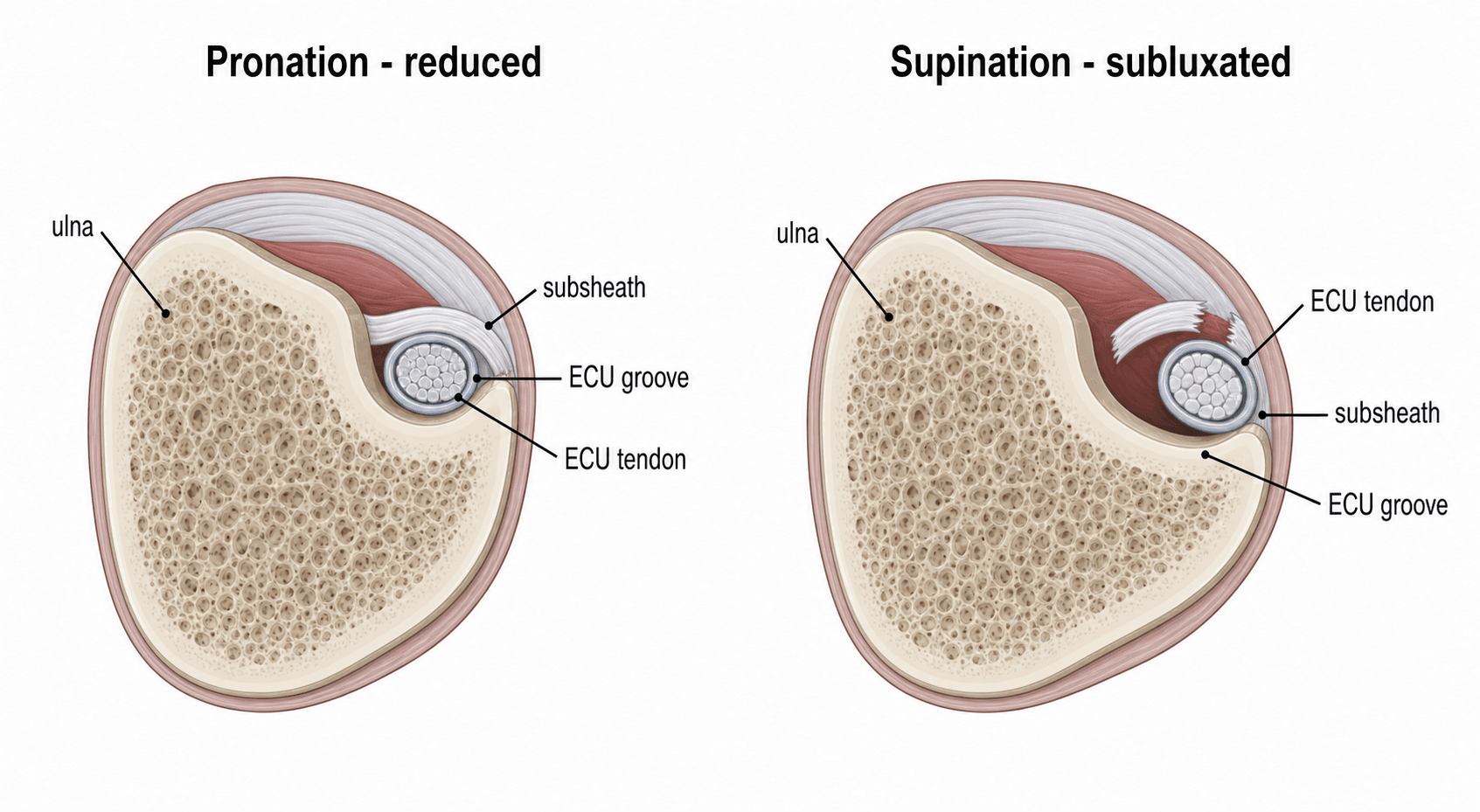
- When the SUBSHEATH is TORN or attenuated, the ECU SUBLUXATES or DISLOCATES out of its groove - typically VOLARLY/ULNARLY - during forearm SUPINATION, ulnar deviation and wrist flexion, and reduces back into the groove on pronation; this produces a painful, often visible/palpable SNAPPING at the dorsoulnar wrist.
- It is classically a sporting injury from a forceful or repetitive SUPINATION-ULNAR DEVIATION-FLEXION load (tennis, golf, racquet and bat sports), but also occurs degeneratively and in rheumatoid disease; it is an important and under-recognised cause of ULNAR-SIDED WRIST PAIN.
- DIAGNOSIS is largely clinical: reproduce the snapping with the provocative manoeuvre (active SUPINATION with ULNAR DEVIATION and flexion, watching/palpating the ECU jump out of its groove), and use the ECU SYNERGY TEST (resisted radial abduction of the thumb with the forearm supinated reproduces dorsoulnar pain) to localise the ECU; DYNAMIC ULTRASOUND (during supination/pronation) best demonstrates the subluxation, and MRI shows subsheath disruption and tendinopathy.
- IMAGING INSTABILITY IS NOT THE SAME AS DIAGNOSING IT. Comparing 41 symptomatic wrists with 64 asymptomatic wrists scanned for an unrelated synovial cyst, there was NO significant relationship between being symptomatic and the degree of ECU instability on MRI, nor with the forearm rotation used during the scan - the authors concluding that ECU instability on MRI is NOT a specific finding. Imaging therefore confirms a mechanism in a patient whose history and examination already implicate the ECU; it cannot by itself establish the tendon as the pain source, and operating on a scan report in a wrist whose symptoms were never reproduced is the error this guards against.
- THE ECU SYNERGY TEST ANSWERS A DIFFERENT QUESTION from the scan - is the pain EXTRA-articular (ECU) or INTRA-articular (TFCC, lunotriquetral, ulnocarpal)? In the original 55-patient series every one of the 21 patients with a NEGATIVE test and an intra-articular-looking examination proved to have intra-articular pathology, and all 11 with a POSITIVE test and an otherwise normal examination got over 90% relief from an ECU sheath injection. But of 22 with a positive test AND intra-articular signs, 10 of the 17 who responded to injection recurred and 6 had ulnocarpal pathology - so a positive test does NOT exclude a second diagnosis. Measured against sonographic abnormality its sensitivity was 73.7% and specificity 85.7% (PPV 82.4%, NPV 78.3%).
- A DIAGNOSTIC LOCAL-ANAESTHETIC INJECTION into the ECU SHEATH is what turns a localising sign into an answer: substantial relief supports the ECU, while persistent pain - or pain returning on lunotriquetral ballottement or TFCC compression - points to intra-articular pathology that treating the tendon will not fix. Test plus injection together reduce the need for MRI and diagnostic arthroscopy.
- It must be distinguished from the other causes of ULNAR-SIDED WRIST PAIN - TFCC tears, DRUJ instability/arthritis, lunotriquetral instability, ulnar impaction and pisotriquetral arthritis.
- MANAGEMENT: acute cases can be treated CONSERVATIVELY with IMMOBILISATION in a long-arm cast/splint in PRONATION and slight wrist extension/radial deviation (the position that reduces and rests the ECU) for several weeks, plus activity modification and NSAIDs; SURGERY is indicated for chronic, recurrent or refractory instability - REPAIR of the subsheath (acute) or RECONSTRUCTION (chronic) using a slip of EXTENSOR RETINACULUM, a periosteal flap or DRUJ capsule, sometimes with ulnar GROOVE-DEEPENING - while corticosteroid injection is reserved for tendinopathy, not for instability.
- “ECU = 6th compartment in its own SUBSHEATH on the dorsal ulnar groove; subsheath tear -> subluxation.
- “Snapping/subluxation provoked by SUPINATION + ulnar deviation + flexion; reduces on pronation. Dynamic ultrasound is the key test.
- “Acute: immobilise in PRONATION/slight extension. Chronic/recurrent: subsheath repair or reconstruction (retinaculum/periosteum/DRUJ capsule) +/- groove deepening.
- “MRI instability is NOT specific: no relationship with symptoms across 41 symptomatic vs 64 asymptomatic wrists. The scan confirms a mechanism; it does not make the diagnosis.
- “Synergy test separates EXTRA- from INTRA-articular: sens 73.7%, spec 85.7%, PPV 82.4%, NPV 78.3%. A positive test does not exclude a coexisting TFCC/LT problem.
- “Diagnostic ECU sheath injection is the step that confirms the source - relief supports ECU; persistent pain on LT ballottement or TFCC compression points intra-articular.
A torn subsheath lets the ECU jump out of its ulnar groove on supination/ulnar deviation/ flexion and snap back on pronation - painful, often visible/palpable.
Reproduce the snap with the provocative manoeuvre; dynamic ultrasound during supination/ pronation shows the subluxation; MRI shows subsheath disruption/tendinopathy.
Anatomy & Mechanism
The ECU occupies the sixth dorsal compartment, where it sits in a bony groove on the dorsal ulnar head held by a dedicated fibro-osseous subsheath - a structure separate from the overlying extensor retinaculum. During forearm rotation the ECU must stay in this groove; the subsheath is the key restraint. A forceful or repetitive load in SUPINATION, ULNAR DEVIATION and wrist FLEXION (as in racquet/bat sports) can tear or stretch the subsheath, after which the ECU subluxates/dislocates out of the groove - usually toward the volar-ulnar side - during supination and reduces on pronation, snapping painfully each time. Chronic/degenerative attenuation and rheumatoid disease can do the same.
The ECU Is a DRUJ Stabiliser - Why It Coexists With DRUJ/TFCC Injury
TFCC tears and DRUJ instability are not merely conditions to exclude - they are linked to ECU instability by a shared functional anatomy, because the ECU is more than a wrist extensor.
The ECU is a dynamic stabiliser of the distal radioulnar joint, most importantly in supination - the position in which the DRUJ is least bony-stable and the ECU and its subsheath resist dorsal-ulnar translation. The floor of the sixth-compartment subsheath blends with the dorsal TFCC/DRUJ capsule, so the structures are anatomically continuous.
A forceful supination injury can damage the subsheath, the TFCC and the DRUJ together - ECU instability, TFCC tears and DRUJ instability frequently coexist rather than being mutually exclusive. So "exclude TFCC/DRUJ" is better read as "also look for them": assess and address all, because isolated ECU surgery may fail if a TFCC tear or DRUJ instability is missed (their treatment is covered in those topics).
The ECU dynamically stabilises the DRUJ (most in supination) and its subsheath floor is continuous with the TFCC/DRUJ capsule - so ECU instability, TFCC tears and DRUJ instability often coexist. Don't treat one and miss the others.
Predisposing Anatomy and Getting the Reconstruction Right
Groove deepening is added when the groove is shallow, and the repair is reinforced to reduce recurrence - which raises the predisposition itself and what the reconstruction is actually trying to restore.
The depth of the ulnar (ECU) groove varies anatomically - a shallow, flat or convex groove predisposes to recurrent subluxation because the bony restraint is weak. This is the rationale for adding ulnar groove-deepening at surgery when the groove is shallow.
The subsheath - not the overlying extensor retinaculum - is the primary restraint, so the goal of repair or reconstruction is to recreate a competent subsheath floor that holds the tendon in the groove. The constructs (a slip of extensor retinaculum, a periosteal flap, or the dorsal DRUJ capsule) must restore that restraint without over-tightening - the tendon must still glide.
A shallow/flat ECU groove predisposes to recurrence -> deepen it; the reconstruction must recreate the subsheath floor (not merely the retinaculum) without strangling tendon glide. Immobilise acute cases in pronation, then rehabilitate progressively - athletes back at a few months, recurrence lower with a reinforced construct.
Assessment & Diagnosis
The diagnosis is mainly clinical. Reproduce the instability with the provocative manoeuvre - active supination with ulnar deviation and wrist flexion - watching and palpating the ECU jump out of its groove, then relocate on pronation. The ECU SYNERGY TEST (with the elbow flexed and forearm supinated, the patient radially abducts the thumb against resistance, which co-contracts the ECU and reproduces dorsoulnar pain) helps localise the ECU as the pain source. DYNAMIC ULTRASOUND through supination and pronation is the best way to demonstrate the subluxation itself in real time, and MRI shows the disrupted subsheath, ECU position and any tendinopathy - but note that showing the tendon move is a different question from proving it is the source of the pain, and imaging alone does not settle the second. Also look for the other causes of ulnar-sided wrist pain - TFCC tears, DRUJ instability or arthritis, lunotriquetral instability, ulnar impaction and pisotriquetral arthritis - which coexist with ECU instability at least as often as they replace it.
What a Positive Test and a Positive Scan Actually Mean
Imaging Instability Is Not the Same as Diagnosing It
A scan that shows the ECU sitting outside its groove is a weaker piece of evidence than it looks. According to PubMed, in a study comparing 41 symptomatic wrists against 64 asymptomatic wrists scanned for an unrelated reason (a synovial cyst, with no ulnar-sided pain), there was no significant relationship between being symptomatic and the degree of instability on MRI, nor with the forearm rotation used during the scan. The authors' conclusion was blunt: ECU instability on MRI is not a specific finding, and detecting it may have nothing to do with the patient's symptoms.
The practical consequence is that the imaging confirms a mechanism in a patient whose history and examination already point to the ECU - it does not, on its own, establish that the ECU is the source of the pain. Operating on a scan report in a wrist whose symptoms were never reproduced by the provocative manoeuvre is the error this finding warns against. Some degree of ECU translation on rotation is common in normal wrists.
The ECU Synergy Test: What It Distinguishes, and How Well
The synergy test was described to answer a specific question in chronic dorsal ulnar-sided wrist pain: is the problem extra-articular (the ECU) or intra-articular (TFCC, lunotriquetral, ulnocarpal)? It works by applying isolated tension to the ECU without loading those other structures.
In the original series of 55 patients with more than four months of dorsal ulnar-sided wrist pain, the test separated the groups cleanly:
- Findings
- The ECU is not the problem
- Outcome
- ALL 21 had ulnar-sided intra-articular pathology on MRI or arthroscopy
- Findings
- Isolated ECU pathology
- Outcome
- ALL had more than 90% pain relief after ECU sheath injection; MRI confirmed isolated ECU tendonitis in 5 of the 6 who were imaged
- Findings
- Both may be present
- Outcome
- 17 of 22 had more than 90% relief after injection, but 10 of those recurred and 6 proved to have ulnocarpal pathology - a positive test does not exclude a second diagnosis
Its measured performance against sonographic ECU abnormality, in 40 wrists with chronic dorsal ulnar-sided pain, was sensitivity 73.7%, specificity 85.7%, positive predictive value 82.4% and negative predictive value 78.3% - useful, and better at ruling in than ruling out, but not decisive on its own.
The Diagnostic Injection
Pairing the test with a local anaesthetic injection into the ECU sheath is what converts a localising sign into an answer, and it is the step the original algorithm turns on. Substantial relief supports the ECU as the pain source; persistent pain, or pain that returns with lunotriquetral ballottement or TFCC compression, points to intra-articular pathology that will not be fixed by treating the tendon. Used this way the test and injection together reduce the need for MRI and diagnostic arthroscopy.
The synergy test and the sheath injection ask is the ECU the source of the pain? Dynamic ultrasound asks does the tendon leave its groove? A patient can answer yes to the second and no to the first, because instability on imaging is common in wrists that do not hurt. Only when the history, the reproduced snap and the imaging agree is the diagnosis secure - and only then should a subsheath be reconstructed.
Management
- Acute / first presentation: CONSERVATIVE treatment - immobilise in a long-arm cast or splint in PRONATION with slight wrist extension/radial deviation (the position that reduces and rests the ECU) for several weeks, with NSAIDs and activity modification; many acute cases settle.
- Tendinopathy/tenosynovitis (no instability): rest, splinting and a corticosteroid injection within the sheath can help - but a steroid injection does NOT treat instability.
- Chronic / recurrent / refractory instability: SURGERY -
- Subsheath REPAIR for an acute/repairable subsheath.
- Subsheath RECONSTRUCTION for chronic cases, using a slip of extensor retinaculum, a periosteal flap (Schlesinger), or the DRUJ dorsal capsule (preserving the extensor retinaculum).
- Ulnar groove deepening may be added when the groove is shallow. Reinforcement of the repair/reconstruction reduces recurrence and, in athletes, allows return to sport at a few months.
Mnemonics & Memory Aids
SNAP
Hook:The ECU SNAPs out in Supination and relocates in Pronation.
6th
Hook:6th compartment, Subsheath, Ultrasound, Repair/Reconstruct.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A tennis player has painful snapping on the ulnar side of the wrist when they supinate. What is the likely diagnosis, and how would you confirm it?”
“How would you manage ECU instability, conservatively and surgically?”
Anatomy & mechanism
- ECU in 6th dorsal compartment in its OWN subsheath, in a dorsal ulnar groove
- Subsheath tear -> ECU subluxates (volarly) on supination/ulnar deviation/flexion
- Athletic (racquet/bat) load; also degenerative/rheumatoid
Diagnosis
- Provocative supination + ulnar deviation/flexion reproduces the snap
- ECU synergy test reproduces dorsoulnar pain: sens 74%, spec 86%, PPV 82%, NPV 78%
- Dynamic ultrasound shows the tendon leaving the groove; MRI shows subsheath/tendinopathy
- MRI instability is NOT specific - no link with symptoms (41 symptomatic vs 64 asymptomatic)
- Diagnostic ECU sheath injection confirms the tendon as the pain source
- Also look for TFCC/DRUJ/LT/ulnar impaction - they coexist rather than exclude
Conservative
- Acute: long-arm immobilisation in PRONATION + slight extension/radial deviation
- Activity modification, NSAIDs
- Steroid injection for tendinopathy only (not instability)
Surgical
- Acute: subsheath repair
- Chronic/recurrent: subsheath reconstruction (retinaculum/periosteum/DRUJ capsule)
- +/- ulnar groove deepening; reinforce to reduce recurrence
Evidence & Key Studies
Recurrent dislocation of the extensor carpi ulnaris tendon in a water-polo athlete
- ECU dislocation/subluxation is rare in the general population but common in athletes whose wrists undergo forceful rotational movements.
- Pain and a snapping sensation at the dorsoulnar wrist, especially during supination, are the predominant symptoms and often need surgery.
- Direct subsheath repair reinforced with an extensor retinaculum graft resolved recurrent dislocation and allowed return to high-level sport at four months.
A novel technique using the dorsal capsule of the DRUJ for ECU subsheath reconstruction
- Symptomatic recurrent ECU subluxation is an increasingly recognised cause of ulnar-sided wrist pain that usually requires subsheath reconstruction.
- Reconstruction using the dorsal DRUJ capsule (preserving the extensor retinaculum) gave mostly satisfactory short-term outcomes (Modified Mayo Wrist Score) in 7 patients.
- It is offered for patients failing conservative treatment or primary repair, and can salvage failed procedures while protecting extensor tendon function.
The ECU synergy test: an aid to diagnose ECU tendonitis
- In 55 patients with more than four months of dorsal ulnar-sided wrist pain, all 21 with a negative synergy test and an examination suggesting intra-articular pathology were confirmed to have it on MRI or arthroscopy.
- All 11 with a positive test and an otherwise normal examination obtained more than 90% relief from an ECU sheath injection, with MRI confirming isolated ECU tendonitis in 5 of the 6 imaged.
- Of 22 with a positive test plus signs of intra-articular pathology, 17 responded to injection but 10 recurred and 6 proved to have ulnocarpal pathology - so the test distinguishes extra-articular from intra-articular pain without excluding a second diagnosis, and forms part of an algorithm that reduces the need for MRI and diagnostic arthroscopy.
Diagnostic performance of the ECU synergy test to detect sonographic ECU abnormalities in chronic dorsal ulnar-sided wrist pain
- Forty wrists with chronic dorsal ulnar-sided wrist pain were assessed with the synergy test and sonography.
- Sensitivity was 73.7%, specificity 85.7%, positive predictive value 82.4% and negative predictive value 78.3% for detecting sonographic ECU abnormality.
- Results differed significantly between wrists with and without ECU abnormality, with no difference by age, sex or symptom duration - supporting the test as a useful provocative manoeuvre rather than a definitive one.
Is it really safe to evaluate symptomatic extensor carpi ulnaris tendon instability by MRI?
- Wrist MRIs of 41 symptomatic patients were compared with 64 asymptomatic wrists imaged for an unrelated synovial cyst, measuring ulnar groove depth and width and the position of the ECU relative to the groove.
- There was no significant relationship between being symptomatic and the degree of instability, nor with the forearm rotation used during the scan.
- The authors conclude that ECU instability on MRI is not a specific finding and its detection may not be related to the patient's symptoms.
The athletic mechanism, the supination-provoked dorsoulnar snapping and the repair-plus-retinaculum-graft technique come from the cited Stathopoulos case, and the recognition of recurrent ECU subluxation as a cause of ulnar-sided wrist pain and the need for subsheath reconstruction (with options preserving the retinaculum) from the cited Png series. The purpose and behaviour of the synergy test, the three-group breakdown and the diagnostic-injection algorithm are Ruland and Hogan; its sensitivity 73.7%, specificity 85.7%, PPV 82.4% and NPV 78.3% are Sato. The finding that instability on imaging does not track with symptoms - and therefore cannot by itself make the diagnosis - is Ozturk, and applies specifically to MRI in that study rather than to dynamic ultrasound, for which no equivalent asymptomatic-comparison data were identified.
Immobilisation is described as lasting several weeks because no verified duration was identified; the position matters more than a precise number of weeks, and the principle is to hold the tendon reduced until the subsheath has healed. The 6th-compartment and subsheath anatomy, the provocative manoeuvre and the conservative-then-surgical sequence are standard hand-surgery teaching. (See also Dorsal Wrist Extensor Compartments, TFCC Injuries, Lunotriquetral Instability, Ulnar Impaction Syndrome and DRUJ Arthritis; no dedicated ulnar-sided-wrist-pain or DRUJ-instability topic exists in the library, so those differentials are named here rather than deferred.)