Abnormal Caudal Fixation of the Spinal Cord
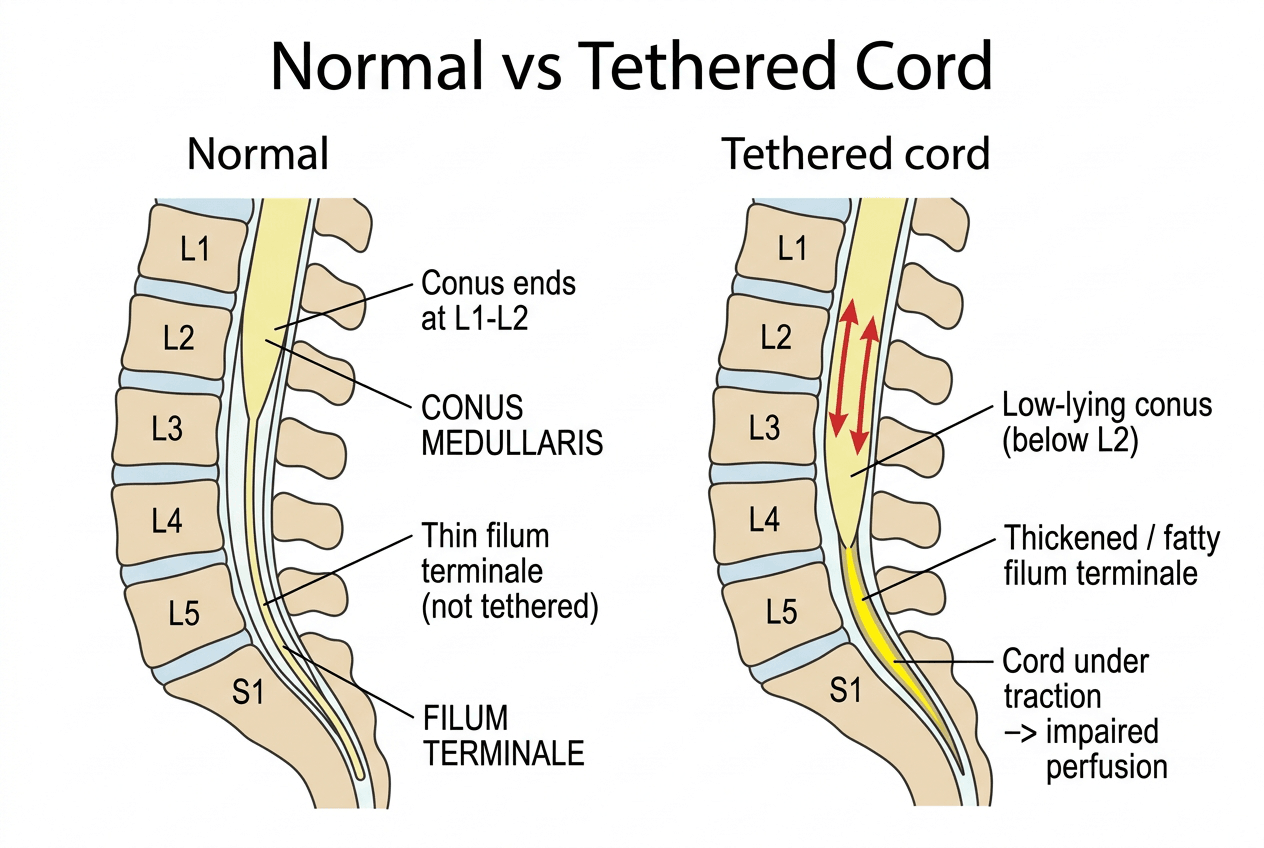
- Tethered cord syndrome is the clinical syndrome produced by abnormal CAUDAL FIXATION (tethering) of the spinal cord, classically a LOW-LYING CONUS MEDULLARIS (ending below the normal L1-L2 level) with a THICKENED and often FATTY FILUM TERMINALE; the fixed, stretched distal cord suffers traction and impaired perfusion, which produces progressive symptoms, often precipitated or worsened by growth (in children) or by flexion/activity.
- The orthopaedic surgeon is often the first to suspect it, because the presenting clues are frequently MUSCULOSKELETAL: a unilateral or progressive CAVOVARUS foot, asymmetric calf/leg ATROPHY or a leg-length discrepancy, and SCOLIOSIS (especially atypical or left thoracic curves, or any curve with a neurological deficit) - so these findings should prompt a search for an underlying tethered cord.
- CUTANEOUS STIGMATA over the lumbosacral midline are an important external marker of underlying spinal dysraphism and tethering: a sacral DIMPLE (especially a large or high one), a HAIRY PATCH (hypertrichosis), a subcutaneous LIPOMA, a haemangioma/capillary malformation or a dermal sinus - their presence should raise suspicion and prompt imaging.
- Symptoms are PROGRESSIVE across three domains: NEUROLOGICAL (lower-limb weakness, sensory change, reflex changes), UROLOGICAL/bowel (neurogenic bladder, incontinence, recurrent urinary infection - a key reason for urological assessment), and PAIN (back and leg pain), and in children the deterioration is often linked to growth spurts.
- MRI is the key investigation, demonstrating the LOW-LYING CONUS (below L2), a THICKENED filum terminale (a thickened/fatty filum, with a filum thickness threshold around 1.3 mm and over being associated with tethering/filum lipoma in studies), and any associated dysraphic lesion (lipomyelomeningocoele, dermal sinus, split-cord malformation, diastematomyelia); spinal ultrasound can screen infants before the posterior elements ossify.
- Treatment is surgical UNTETHERING - releasing the tethering element, most simply by sectioning a tight/thickened filum terminale (or addressing a more complex lesion) - performed to halt progression and, where possible, improve symptoms; the principle is that established deficits may not fully reverse, so timely surgery in a symptomatic or deteriorating patient is important, ideally within a multidisciplinary (neurosurgery, urology, orthopaedics) framework.
- “Tethered cord = abnormal caudal fixation: LOW conus (below L2) + THICKENED/fatty filum -> traction/ischaemia -> progressive neuro/uro/pain symptoms.
- “ORTHOPAEDIC clues: unilateral CAVOVARUS foot, asymmetric leg atrophy/leg-length difference, scoliosis (atypical/neurological). Plus cutaneous stigmata (dimple, hairy patch, lipoma).
- “MRI confirms (low conus, thick filum); treat by surgical UNTETHERING (filum section). Halts progression - established deficits may not fully reverse.
A unilateral/progressive cavovarus foot, asymmetric leg atrophy, scoliosis, and lumbosacral cutaneous stigmata (dimple, hairy patch, lipoma) - especially with bladder symptoms.
MRI: low conus (below L2), thickened/fatty filum. Untether for documented deterioration, not for the scan alone - it halts progression, but the scoliosis often does not stop.
Definition, Clues & Imaging
Tethered cord syndrome is the syndrome of abnormal caudal fixation of the spinal cord - a low-lying conus (below L1-L2) with a thickened, often fatty filum terminale - so the distal cord is under traction with impaired perfusion, producing progressive symptoms, often worsened by growth. The orthopaedic surgeon frequently suspects it from the periphery: a unilateral or progressive cavovarus foot, asymmetric calf atrophy or a leg-length difference, and scoliosis (especially atypical or neurological curves). Lumbosacral cutaneous stigmata - a sacral dimple, hairy patch, lipoma, haemangioma or dermal sinus - are an important external marker. Symptoms span neurological, urological and pain domains. MRI confirms the low conus and thickened filum and defines any dysraphic lesion; spinal ultrasound screens infants.

What Tethers the Cord: Classifying the Lesions
The tethering lesions - thickened or fatty filum, lipomyelomeningocoele, dermal sinus, split-cord - are best organised into a causal spectrum, because the cause determines the operation and the risk of re-tethering.
- Tight/thickened filum terminale (often a fatty filum / fibrolipoma) - the simplest, sectioned at surgery.
- Spinal lipomas - lipomyelomeningocoele and intradural/dorsal/terminal lipomas.
- Dermal sinus tract (with or without a dermoid/epidermoid).
- Split-cord malformation (diastematomyelia).
- Others: terminal myelocystocele, meningocoele manque, caudal regression.
Scar tethering after prior surgery - most importantly re-tethering after a myelomeningocoele repair (or other spinal surgery), a common cause of late deterioration in repaired spina bifida: symptomatic tethering developed in 23 percent of one long-term cohort of children who had neonatal closure. Different lesions, one syndrome.
The open dysraphisms and the individual tethering lesions are developed separately in myelomeningocele, spina bifida, split-cord malformation and caudal regression syndrome; an associated syringomyelia should be looked for on the same MRI.
Pathophysiology: Why Traction Damages the Cord (and Why Untethering Helps)
The cord is under traction with impaired perfusion, and untethering halts progression. The mechanism linking traction to dysfunction is what explains why early release can recover recent symptoms.
A normal filum terminale is elastic and lets the cord glide with flexion/extension and growth; a tight/thickened (often fatty) filum loses that elasticity and instead transmits tension to the conus. The stretched distal cord then suffers impaired oxidative metabolism: experimental work (Yamada) showed traction reduces mitochondrial oxidative metabolism (cytochrome-oxidase redox changes) and blood flow in the lumbosacral cord.
Because it is a reversible metabolic/ischaemic dysfunction (not simple mechanical transection), symptoms worsen with anything that increases tension - growth spurts, flexion, activity - and early untethering can REVERSE the metabolic dysfunction and recover recent deficits, whereas long-standing structural damage may be fixed. This is the rationale for timely surgery.
Tethered cord syndrome is a reversible metabolic/ischaemic dysfunction of the traction-stretched conus (Yamada) - which is why it progresses with tension/growth and why timely untethering can recover recent deficits while established damage may not reverse.
Management
- Confirm and characterise on MRI - the low conus, thickened/fatty filum and any associated lesion (lipomyelomeningocoele, dermal sinus, split-cord/diastematomyelia); ultrasound screens infants before the posterior elements ossify.
- Assess all three domains - neurological examination, urological assessment (urodynamics/bladder), and the orthopaedic deformities (foot, leg, spine).
- Surgical untethering - release the tethering element, most simply by sectioning a tight/thickened filum terminale, or addressing a more complex lesion; the aim is to halt progression and, where possible, improve symptoms. The trigger is documented clinical or urodynamic deterioration, not the MRI appearance - in a repaired myelomeningocoele radiological tethering is near-universal, and an incidental fatty filum in an asymptomatic child with normal examination and urodynamics is surveyed, not sectioned.
- Act before deficits become fixed - established neurological/urological deficits may not fully reverse, so timely surgery in a symptomatic or deteriorating patient matters; manage within a multidisciplinary team (neurosurgery, urology, orthopaedics).
The recurring orthopaedic lesson of tethered cord syndrome is that a unilateral cavovarus foot, asymmetric leg atrophy, or an atypical/neurological scoliosis is frequently the FIRST sign of an underlying tethered cord, so these findings - especially with lumbosacral cutaneous stigmata or any bladder symptoms - should prompt a neuro-axis MRI rather than treating the foot or curve in isolation. Operating on the foot or spine without recognising and addressing the tethered cord risks ongoing progression and poorer outcomes. Because the syndrome is progressive and established deficits may not fully reverse, timely untethering in a symptomatic or deteriorating patient, coordinated with neurosurgery and urology, is the priority.
Who Actually Needs Untethering - and What It Delivers
Saying that treatment is untethering leaves the harder question unanswered: untether whom, and on what trigger? The answer is not the MRI appearance.
In a repaired myelomeningocoele the cord is radiologically tethered in almost everyone - the placode is scarred to the dural repair by definition - so a low conus on MRI is an expected postoperative finding, not an indication. Release is offered for documented clinical or urodynamic deterioration: new or progressive lower-limb weakness, increasing spasticity or contracture, gait change, a progressing or new scoliosis, back or leg pain, or a deteriorating bladder. Operating on the scan alone commits a child with a normal trajectory to a re-operation through scar. In the closed dysraphisms an incidental fatty filum found on imaging performed for another reason, in a child with no symptoms, no urodynamic abnormality and normal examination, is likewise watched rather than sectioned, with surveillance of examination, growth, curve and bladder.
A distinct group has the clinical and urodynamic picture of tethering but a conus in a normal position on MRI - occult tethered cord syndrome. Uncontrolled series are enthusiastic: in 60 children (aged 3-18, mean follow-up 13.9 months) selected on strict criteria, urinary incontinence or retention resolved completely in 52 percent and markedly improved in a further 35 percent, faecal incontinence resolved in 56 percent, and weakness, sensory change and pain improved or resolved in all. But the only randomised comparison - filum section plus medical treatment versus medical treatment alone in children refractory to a year of conservative management with a normal conus and abnormal urodynamics - found no significant difference in urodynamic score, bowel-and-bladder dysfunction score or quality of life at one year. That trial accrued only 21 patients over 8 years, and its own interim analysis calculated that more than 700 per arm would be needed to show a urodynamic difference of the size observed - so it is a genuinely underpowered null, not proof that the operation fails. The defensible examination answer is that the entity exists as a clinical description but its surgical indication is unproven, and that the null result is what a candidate should be able to quote rather than the uncontrolled improvement rates alone.
Long-term single-institution follow-up of the myelomeningocoele population (mean 12 years) ranks the response by symptom: pain responds best - improved in 100 percent; lower-limb strength improved in 70 percent on three-month manual muscle testing; bladder function improved in 64 percent; spasticity improved in about two-thirds; and lower-limb contractures were, as expected, merely stable (78 percent) rather than improved. Counsel by domain, not with a single global figure.
In the same cohort scoliosis still progressed after untethering in 52 percent, and 28 percent went on to need spinal fusion. Untethering reliably relieves pain; it does not guarantee that a neuromuscular curve will stabilise. Promising a family that releasing the cord will settle the spine over-reads the evidence - the curve continues to be managed in its own right.
Re-tethering is common enough to be part of the consent, not a footnote. Of 114 children who developed symptomatic tethering after myelomeningocoele closure, 33 (29 percent) required more than one untethering, for 163 procedures across 114 patients - so recurrence should be quoted as roughly one in three needing further surgery over a decade of follow-up, and lifelong surveillance is the corollary.
Mnemonics & Memory Aids
TETHER
Hook:TETHER: Thick filum/low conus, External skin stigmata, Toes (cavovarus), Hold of bladder lost, Examine/MRI, Release (untether).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child has a unilateral cavovarus foot and a sacral dimple. What underlying diagnosis must you consider and how do you investigate?”
“How is tethered cord syndrome managed, and what do you tell the family about outcome?”
Definition
- Abnormal caudal fixation of the cord (traction/ischaemia)
- Low-lying conus (below L2) + thickened/fatty filum terminale
- Progressive; often worsened by growth
Clues
- Orthopaedic: unilateral cavovarus foot, asymmetric leg atrophy/leg-length, scoliosis
- Cutaneous: sacral dimple, hairy patch, lipoma, haemangioma, dermal sinus
- Urological: neurogenic bladder, incontinence, recurrent UTI
Diagnosis
- MRI: low conus, thickened/fatty filum, associated dysraphic lesion
- Spinal ultrasound screens infants (before ossification)
- Urodynamics for bladder assessment
Management
- Surgical untethering (section the filum / release the lesion)
- Indication is documented clinical/urodynamic deterioration, NOT a low conus on MRI
- Halts progression; established deficits may not fully reverse - act timely
- Outcomes by domain: pain 100%, strength 70%, bladder 64%; scoliosis still progressed in 52% (28% fused)
- Re-tethering in about 29% (more than one operation); lifelong surveillance
- Occult TCS (normal conus): the one RCT was null and underpowered - indication unproven
- Multidisciplinary; manage foot/spine/bladder in their own right
Evidence & Key Studies
Cutaneous markers and filum terminale thickness in identifying tethered cord (children with sacral dimples)
- In children with sacral dimples, tethered cord syndrome requiring surgery was identified in 4.6%, supporting the link between lumbosacral cutaneous markers and underlying tethering.
- A dimple long diameter of 5 mm or more was significantly associated with tethered cord syndrome.
- A filum terminale thickness cutoff of 1.3 mm or more predicted filum terminale lipoma with about 93% sensitivity and 80% specificity, and spinal ultrasound can screen for it.
Surgical management of tethered spinal cord through a minimally invasive approach (filum release)
- Tethered cord release can be performed by hemilaminectomy, durotomy and careful separation/sectioning of the filum terminale, here via a minimally invasive approach.
- The case (a young adult with chronic back pain and thigh numbness) had a midline fusion defect and abnormal conus medullaris termination, illustrating the typical pathology.
- Postoperative recovery was rapid without complications, illustrating the principle of untethering to relieve traction on the cord.
Tethered cord release: long-term outcomes, by symptom domain, in 114 patients
- Single-institution cohort of 502 children who had myelomeningocoele closure between 1975 and 2008: symptomatic tethering developed in 114 (23 percent); mean follow-up 12 years (range 1 month to 23.3 years).
- Shunt malfunction is the commonest cause of decline in these children; symptomatic tethering is second - so a new deficit is not automatically the cord.
- Response ranked by domain: pain improved in 100 percent, lower-limb strength in 70 percent at 3 months, bladder function in 64 percent, spasticity in about two-thirds; contractures were stable (78 percent) rather than improved.
- Scoliosis progressed after untethering in 52 percent, with 28 percent requiring spinal fusion - untethering does not guarantee curve stabilisation.
- 33 of the 114 (29 percent) needed more than one untethering, for 163 operations in total: re-tethering is common.
- Retrospective, single centre, no control group - the authors state this explicitly.
Filum section for occult tethered cord syndrome: the only randomised comparison was null (and underpowered)
- Randomised controlled pilot: children with urinary incontinence refractory to a year or more of medical management, a NORMAL conus position on MRI and abnormal urodynamics, randomised to filum section plus medical treatment versus medical treatment alone.
- At one year the bowel-and-bladder dysfunction score improved in both arms (20 percent surgical, 24 percent medical) and the urodynamic score barely moved (6 percent and 4 percent); quality-of-life scales improved modestly in both. No difference reached significance.
- Accrual was only 21 patients over 8 years; interim analysis indicated more than 700 patients per arm would be needed to demonstrate a urodynamic difference of the size seen - so this is an underpowered null, not a demonstration of no effect.
- The authors conclude the data challenge the concept of occult tethered cord syndrome as a surgically treatable entity.
The association of lumbosacral cutaneous markers (sacral dimple size) with tethered cord and the filum terminale thickness threshold (around 1.3 mm) with spinal ultrasound screening come from the cited Watanabe study; the surgical principle of untethering by sectioning/separating the filum terminale, and the typical pathology (abnormal conus termination with a dysraphic defect), from the cited Ozer report. The low-conus/thickened-filum definition, the orthopaedic clues (cavovarus foot, asymmetric leg, scoliosis), the neuro/urological/pain symptom triad and the multidisciplinary, progression-halting principle are standard, well-established teaching. The domain-by-domain outcome figures, the scoliosis-progression and fusion rates and the re-tethering rate come from the cited Bowman cohort, which is retrospective, single-centre and uncontrolled and drawn entirely from a repaired-myelomeningocoele population - so those numbers should not be transferred without qualification to a child having a simple fatty filum sectioned. The occult tethered cord randomised result and its power calculation come from the cited Steinbok trial; the uncontrolled improvement rates quoted alongside it are from Wehby and colleagues (60 children, mean follow-up 13.9 months, PMID 15292632). No agreed diagnostic criteria for occult tethered cord syndrome exist, and no threshold of conus level or filum thickness has been shown to identify which asymptomatic child will later deteriorate, so none is offered here. See also spina bifida, myelomeningocele, split-cord malformation, caudal regression syndrome, syringomyelia, cavovarus foot and paediatric cavus foot.