Indolent Granulomatous Infection of a Peripheral Joint
- Skeletal tuberculosis is haematogenous spread of Mycobacterium tuberculosis from a primary (often pulmonary) focus; after the SPINE (Pott's, the commonest site), the next most affected are the WEIGHT-BEARING PERIPHERAL JOINTS - the HIP and KNEE - usually as a chronic, INDOLENT MONOARTHRITIS.
- Presentation is INSIDIOUS: weeks-to-months of joint pain, swelling, stiffness and muscle wasting, often a relatively 'COLD' swelling without the acute heat/redness of pyogenic infection, with low-grade constitutional symptoms (night sweats, weight loss, malaise); diagnosis is frequently DELAYED. A biphasic age pattern is seen - elderly patients in low-incidence countries and YOUNGER patients with a MIGRATION background.
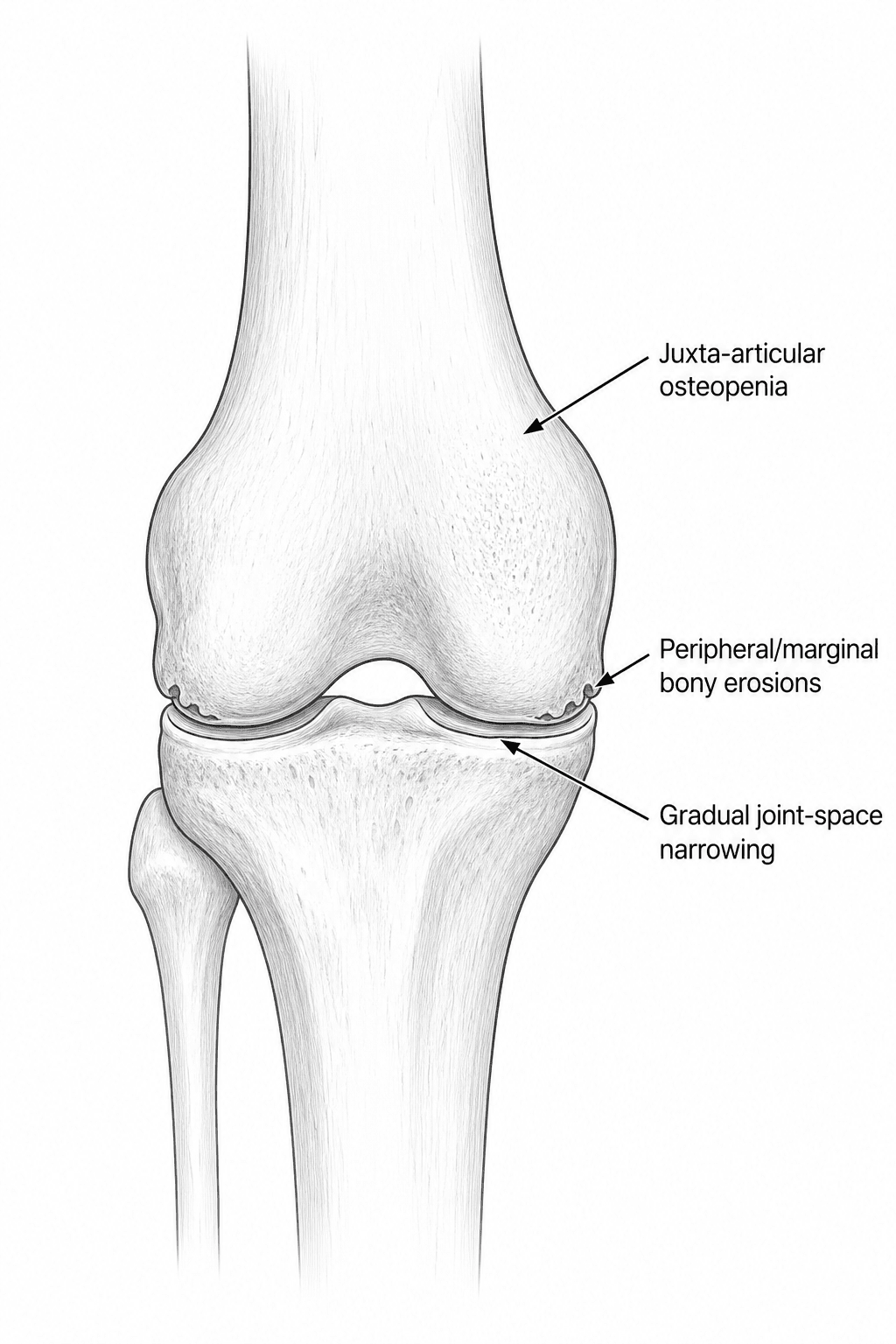
- The classic radiographic PHEMISTER TRIAD is: (1) juxta-articular OSTEOPENIA, (2) PERIPHERAL/marginal bony EROSIONS, and (3) GRADUAL joint-space narrowing - importantly the joint space is RELATIVELY PRESERVED until late, in contrast to PYOGENIC septic arthritis, which destroys cartilage and the joint space rapidly.
- DIAGNOSIS rests on obtaining tissue: SYNOVIAL BIOPSY showing CASEATING GRANULOMAS (the histological hallmark) plus mycobacterial CULTURE (the gold standard but slow - weeks) and rapid molecular tests (NAAT/GeneXpert PCR); synovial fluid is typically lymphocytic with low glucose but AFB smear has low yield. Support with ESR/CRP, tuberculin/IGRA, MRI (extent, abscess) and a chest radiograph.
- The MAINSTAY of treatment is ANTI-TUBERCULOUS CHEMOTHERAPY - standard multi-drug therapy (rifampicin, isoniazid, pyrazinamide, ethambutol intensive phase then rifampicin/isoniazid continuation) - for a PROLONGED course - local protocols commonly specify 9-12 months for bone and joint disease, though in SPINAL tuberculosis six randomised trials found 6 months equivalent to 9 or more (pooled RR 0.98) and no randomised evidence exists for peripheral joints, so the longer course is protocol-driven rather than trial-proven; SURGERY is ADJUNCTIVE (biopsy for diagnosis, drainage of a cold abscess, synovectomy/debridement, and arthrodesis or delayed arthroplasty for end-stage destruction).
- Untreated or late peripheral joint TB destroys the joint and leads to DEFORMITY, fibrous/bony ANKYLOSIS (especially hip and knee) and, in children, growth disturbance/limb-length discrepancy; any arthroplasty for the burnt-out joint should be done once the disease is QUIESCENT and under anti-TB cover because of the reactivation risk.
- “After the spine, hip and knee are the commonest skeletal TB sites; chronic indolent MONOarthritis with a 'cold' joint and constitutional symptoms.
- “Phemister triad: juxta-articular osteopenia + peripheral erosions + LATE joint-space narrowing (joint space preserved early - unlike rapid pyogenic destruction).
- “Diagnose by synovial biopsy (caseating granuloma) + culture (gold standard, slow) + PCR; treat with prolonged anti-TB chemotherapy, surgery adjunctive.
Indolent monoarthritis, 'cold' swelling, constitutional symptoms; joint space preserved until late (Phemister triad). Diagnose by biopsy/culture/PCR; treat with anti-TB drugs.
Acute hot, red, exquisitely painful joint; rapid cartilage/joint-space destruction. A surgical emergency - urgent washout + antibiotics; see septic arthritis pathophysiology.
Pathophysiology & Presentation
TB reaches the joint by haematogenous spread, seeding the synovium or the juxta-articular bone. A granulomatous synovitis forms, producing a pannus that gradually erodes cartilage and bone - but SLOWLY, which is why the joint space is preserved early. The patient develops an insidious monoarthritis of a weight-bearing joint (commonly hip or knee) with pain, swelling, stiffness, muscle wasting and limp, often a relatively cold swelling, plus constitutional features (night sweats, weight loss, low-grade fever). Because it mimics inflammatory or low-grade pyogenic arthritis, diagnosis is often delayed - consider it especially in patients from TB-endemic areas, those with a migration background, and the immunocompromised.
Pathogenesis: Why the Phemister Pattern
- Two routes to the joint. Either primary synovial TB (haematogenous seeding of the vascular synovium -> granulomatous synovitis) or secondary spread from a juxta-articular/epiphyseal osteomyelitic focus that erodes into the joint.
- Why the erosions are peripheral ('kissing lesions'). The granulomatous pannus arises from the synovial reflections and creeps over the cartilage from the joint margins - the peripheral 'bare areas' where synovium contacts bone not covered by cartilage - so marginal/peripheral erosions appear first, often on both opposing sides of the joint ('kissing' lesions); the central weight-bearing cartilage is spared until late, which is why the joint space is preserved early.
- Why it is indolent. Mycobacterial destruction is slow and granulomatous, lacking the proteolytic enzyme load of pyogenic pus - hence the chronic course and the contrast with the rapid cartilage loss of septic arthritis.
- Why the osteopenia. Hyperaemia and disuse of the painful joint produce the juxta-articular osteopenia that completes the triad.
The Phemister triad falls out of the mechanism: a marginal pannus erodes the peripheral bare areas first (peripheral/'kissing' erosions) while sparing the central cartilage (joint space preserved early), the slow granulomatous process keeps it indolent, and disuse/hyperaemia give the juxta-articular osteopenia. Pyogenic arthritis, with proteolytic pus, instead destroys the central joint space fast.
How Long to Treat - the Question Behind 'Prolonged Course'
"Nine to twelve months, follow local protocol" is the safe answer, but the duration of chemotherapy for osteoarticular tuberculosis has been tested, and a candidate who knows what the trials showed - and what they did not cover - answers a level above one who quotes a range.
A systematic review and meta-analysis of six randomised trials (877 patients) comparing 6 months against 9 months or longer in spinal tuberculosis found healing in 375 of 414 (90.6 percent) on the short course against 404 of 463 (87.3 percent) on the long course - pooled relative risk 0.98 (95 percent CI 0.92 to 1.04, p = 0.44), that is, no detectable difference. An earlier literature review found relapse in 0 of 56 treated with 6 months of isoniazid, rifampicin and pyrazinamide against 4 of 218 (2 percent) treated for 9 months or more. Heterogeneity between the trials was substantial (I-squared 40.8 percent), and equivalence within a confidence interval is not proof of equivalence.
Every one of those trials studied spinal disease. No randomised comparison of treatment duration confined to peripheral joint tuberculosis was retrieved, so applying the six-month result to a tuberculous hip or knee is an extrapolation - reasonable, because the organism and the drugs are the same, but an extrapolation nonetheless, and one to declare rather than disguise. National programmes and local protocols still commonly specify 9 to 12 months for bone and joint disease, and drug resistance, HIV co-infection, poor adherence and extensive or multifocal disease all push towards the longer end. Treat to the local protocol; know why the debate exists.
If asked why bone and joint tuberculosis is treated longer than pulmonary disease, say that it is historical practice supported by protocol rather than by trials showing longer is better - in spinal disease six months matched nine or more across six randomised trials, and the evidence specific to peripheral joints is absent, so the longer course persists on the grounds of poor drug penetration into avascular and necrotic bone, difficulty assessing healing, and the consequences of relapse in a weight-bearing joint.
Investigation & Diagnosis
The diagnosis is confirmed on tissue:
- Synovial biopsy - caseating granulomas are the histological hallmark.
- Mycobacterial culture - the gold standard for confirmation and drug sensitivities, but slow (several weeks).
- Molecular tests (NAAT/GeneXpert PCR) - rapid detection of M. tuberculosis and rifampicin resistance.
- Synovial fluid - typically lymphocytic with low glucose; AFB smear has low yield. Supportive tests: raised ESR/CRP, tuberculin (Mantoux) / IGRA, MRI (defines synovitis, abscess, bone and soft-tissue extent), plain radiographs (Phemister triad) and a chest radiograph for pulmonary disease. Always send samples for both histology and culture when sampling, and consider HIV testing.
Differential of the Chronic Indolent (Granulomatous) Monoarthritis
TB is easily contrasted with acute pyogenic arthritis, but the harder task is the differential of a chronic, indolent monoarthritis, since several conditions mimic it. Caseating granuloma plus a positive mycobacterial culture or PCR is what confirms TB.
- Discriminating features
- Indolent, Phemister triad, constitutional symptoms; endemic/migrant/immunocompromised
- The test that separates it
- CASEATING granuloma on synovial biopsy with mycobacterial culture or PCR
- Discriminating features
- Acute hot/red joint, RAPID joint-space destruction
- The test that separates it
- Aspiration: neutrophilic fluid, pyogenic organism on Gram stain and culture
- Discriminating features
- Animal or unpasteurised-dairy exposure, or an endemic area; sacroiliitis and large joints
- The test that separates it
- Brucella serology and blood culture (warn the laboratory - it is a hazard-group pathogen)
- Discriminating features
- Endemic exposure or immunocompromise; indolent granulomatous picture
- The test that separates it
- Fungal culture and histology on tissue - request specifically, it is not routine
- Discriminating features
- Indolent, often hand or tendon-sheath; aquatic exposure or immunocompromise
- The test that separates it
- Mycobacterial culture with speciation - a positive AFB culture is NOT automatically TB
- Discriminating features
- Systemic sarcoid, bilateral hilar nodes
- The test that separates it
- Biopsy shows NON-caseating granuloma - the histological pivot away from TB
- Discriminating features
- Monoarticular RA, JIA or spondyloarthropathy; PVNS; gout or CPPD; synovial tumour
- The test that separates it
- Serology; MRI blooming for haemosiderin; polarised microscopy for crystals; imaging plus biopsy for a mass
Each of these is developed separately in septic arthritis pathophysiology, brucellosis of the spine, fungal osteomyelitis, atypical mycobacterial infection, musculoskeletal sarcoidosis, PVNS, gout and crystal arthropathy and pseudogout and CPPD disease.
A chronic 'cold' monoarthritis is not automatically TB: weigh brucellar, fungal and atypical-mycobacterial infection, sarcoid (non-caseating), monoarticular inflammatory arthritis, PVNS, crystal disease and synovial tumour. The discriminator for TB is caseating granuloma plus a positive mycobacterial culture/PCR - which is exactly why getting tissue (not just aspirate) matters.
Management
- Anti-tuberculous chemotherapy (mainstay): standard multi-drug therapy - an intensive phase of rifampicin, isoniazid, pyrazinamide and ethambutol, then a continuation phase of rifampicin and isoniazid - for a prolonged total course (local and national protocols commonly specify 9-12 months for bone and joint TB; adjust for drug resistance). Doses are weight-based and set by WHO and national programmes - prescribe to the local protocol rather than from memory.
- Surgery (adjunctive): biopsy for diagnosis; drainage of a cold abscess; synovectomy/ debridement of extensive disease or to relieve symptoms; arthrodesis for a painful destroyed joint; and delayed total joint arthroplasty for end-stage destruction - performed once the disease is quiescent and under anti-TB cover to reduce reactivation.
- Supportive: rest/splintage in the acute phase to protect the joint and prevent deformity, then graded rehabilitation; nutritional support; manage comorbidity (HIV, diabetes).
A peripheral joint destroyed by past TB may present years later as a painful, stiff or ankylosed joint requiring arthrodesis takedown or arthroplasty. Reconstructive surgery on a previously tuberculous joint carries a real risk of disease reactivation, so it should be undertaken only when the disease is quiescent, with peri-operative anti-TB cover, and after counselling about reactivation, stiffness and the technical difficulty of operating on scarred, deformed anatomy.
Mnemonics & Memory Aids
PHEMISTER
Hook:Phemister triad = osteoPenia, Erosions, Maintained (late-narrowing) joint space.
COLD JOINT
Hook:TB joint = a COLD JOINT: chronic, lymphocytic, granulomatous, drug-treated.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A young migrant has months of insidious knee pain and swelling with night sweats. How would you investigate and what would the radiograph show?”
“How is peripheral tuberculous arthritis treated, and what are the long-term consequences?”
Epidemiology & presentation
- Skeletal TB: spine (Pott's) most common, then hip & knee (peripheral)
- Indolent monoarthritis, 'cold' swelling, constitutional symptoms; biphasic age (elderly + young migrants)
- Haematogenous granulomatous synovitis -> slow joint destruction
Radiology (Phemister triad)
- Juxta-articular osteopenia
- Peripheral/marginal bony erosions
- Gradual joint-space narrowing (preserved until late) - vs rapid pyogenic destruction
Diagnosis
- Synovial biopsy (caseating granuloma) + culture (gold standard, slow) + PCR (rapid)
- Synovial fluid lymphocytic, low glucose (AFB smear low yield)
- ESR/CRP, IGRA/Mantoux, MRI, CXR, HIV test
Management
- Anti-TB chemotherapy mainstay (RIPE -> RH); protocols specify 9-12 months for bone/joint, doses weight-based
- 6 months matched 9+ months in six RCTs in SPINAL TB (RR 0.98); no randomised data for peripheral joints
- Surgery adjunctive: biopsy, abscess drainage, synovectomy, arthrodesis/delayed arthroplasty
- Sequelae: ankylosis/deformity; reconstruct only when quiescent + anti-TB cover
Evidence & Key Studies
Musculoskeletal tuberculosis revisited: bone and joint tuberculosis
- Sites of musculoskeletal TB were the spine (most common), peripheral joints and soft tissues, with a biphasic age distribution (elderly natives and younger patients with a migration background).
- Diagnosis relied on histology, PCR and culture; many patients required surgery and secondary deformities were frequent (especially spinal disease).
- Musculoskeletal TB should be considered for atypical joint infections or nonspecific bone lesions in younger patients with a migration background or specific risk factors.
Hip fusion takedown with subsequent hip and knee arthroplasty after childhood tuberculosis
- Illustrates a long-term sequela of peripheral joint TB - hip fusion/ankylosis from tuberculosis in adolescence presenting decades later.
- Staged hip fusion takedown with total hip arthroplasty followed by total knee arthroplasty gave a marked improvement in pain and quality of life.
- Reconstruction of a previously tuberculous joint requires careful planning and management of expectations.
Six months versus nine months or longer in SPINAL tuberculosis: a meta-analysis of six randomised trials
- Systematic review and meta-analysis of 8 publications describing 6 randomised trials with at least 1 year of follow-up, comparing 6 months of antitubercular therapy against 9 months or more in SPINAL tuberculosis.
- Healed status was achieved in 375 of 414 patients (90.58 percent) on the short course against 404 of 463 (87.26 percent) on the long course.
- Pooled relative risk 0.98 (95 percent CI 0.92 to 1.04, p = 0.439) - no detectable difference in healing between the two durations.
- Considerable heterogeneity between trials (I-squared 40.8 percent, p = 0.149), and the authors phrase the conclusion as short-course chemotherapy 'may be considered' rather than as an established standard.
- Every included trial studied SPINAL disease; the meta-analysis says nothing directly about peripheral joint tuberculosis, so applying it to a tuberculous hip or knee is an extrapolation.
The distribution of skeletal TB (spine then peripheral joints), the biphasic age pattern and the diagnostic reliance on histology/PCR/culture come from the cited Vielgut study, and the destructive ankylosing sequelae and their late reconstruction from the cited Pobozy report, which is a single case and therefore illustrates a pathway rather than quantifying an outcome. The randomised comparison of treatment duration comes from the cited Aryal meta-analysis, and the relapse figures quoted alongside it (none of 56 on six months against 4 of 218 on nine months or more) from van Loenhout-Rooyackers and colleagues (Int J Tuberc Lung Dis 2002, PMID 11934144), a literature review rather than a trial - and both address SPINAL disease only. No randomised trial of treatment duration confined to peripheral joint tuberculosis was retrieved, and no published relapse rate specific to the tuberculous hip or knee was found, so the durations given here are protocol-based and the six-month evidence is labelled as an extrapolation. First-line drug doses are weight-based and set by WHO and national tuberculosis programmes; no dose schedule specific to osteoarticular disease was retrieved, so none is quoted - prescribe to the local protocol, with resistance testing guiding any deviation. The Phemister triad, the caseating-granuloma histology and the principle of chemotherapy-first management are standard, well-established teaching. See also tuberculosis of the spine (Pott's disease), septic arthritis pathophysiology and atypical mycobacterial infection.