Orthopaedic Relevance
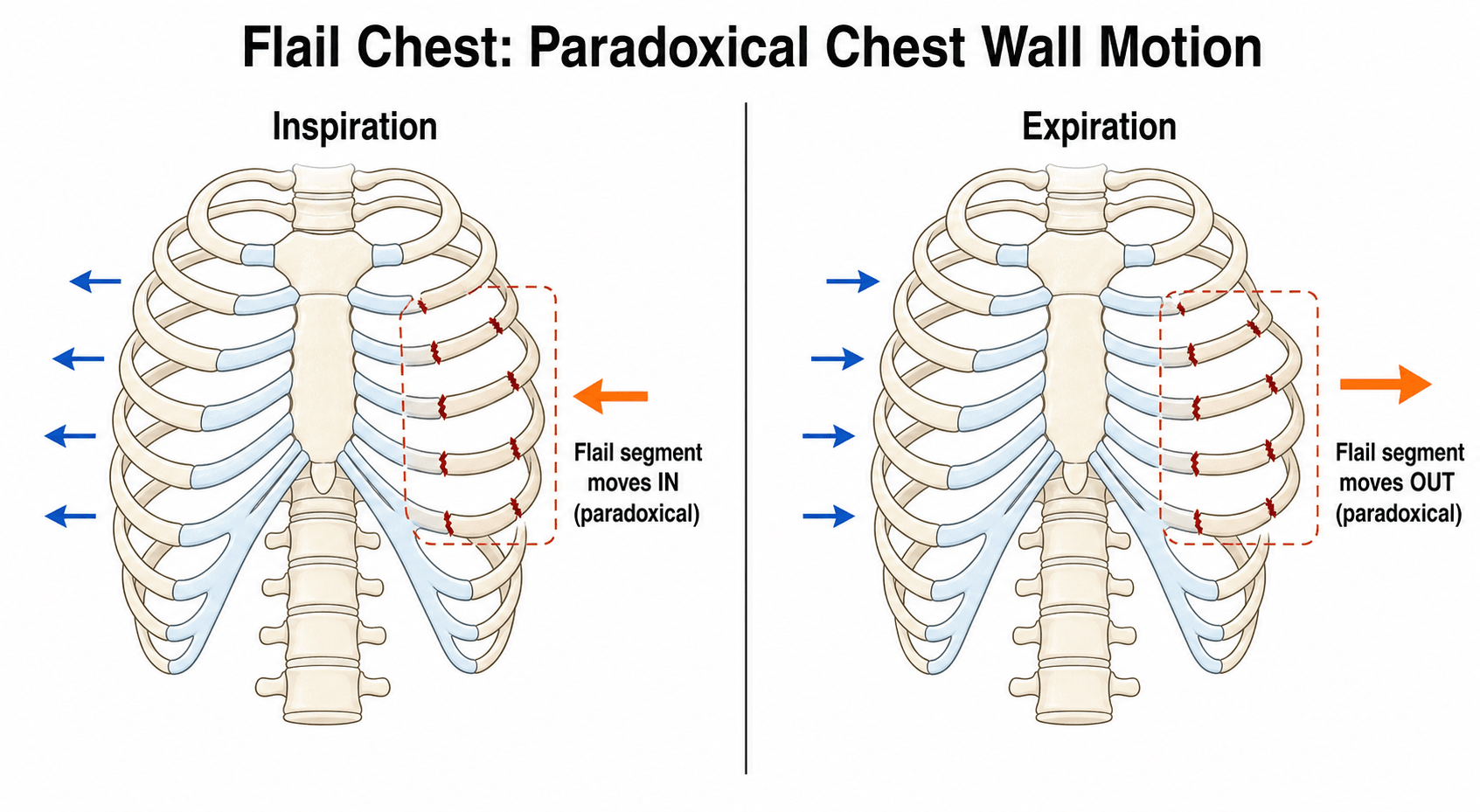
- Flail chest is defined as THREE or more CONTIGUOUS ribs each fractured in TWO or more places, which creates a free 'flail' segment of chest wall that moves PARADOXICALLY - drawn inward during inspiration and pushed outward during expiration - and it is a marker of high-energy chest trauma.
- The crucial physiological point is that the morbidity and mortality of flail chest are driven mainly by the underlying PULMONARY CONTUSION and by PAIN-related chest-wall splinting and HYPOVENTILATION (causing atelectasis, retained secretions, pneumonia and respiratory failure) rather than by the paradoxical motion itself - so the priorities are oxygenation, analgesia and pulmonary care, not merely 'splinting' the segment.
- Initial MANAGEMENT follows ATLS principles (it is a chest injury in a trauma patient) and centres on MULTIMODAL ANALGESIA - including REGIONAL techniques (thoracic epidural, paravertebral or intercostal/erector spinae blocks) - aggressive PULMONARY TOILET and chest physiotherapy, supplemental oxygen, and escalation to non-invasive or invasive ventilatory support when respiratory failure develops; good analgesia that allows deep breathing and coughing is central.
- SURGICAL STABILISATION OF RIB FRACTURES (SSRF) - rib plating/fixation - is increasingly performed and the evidence supports it: in patients with multiple rib fractures and flail chest, SSRF is associated with LOWER MORTALITY (with the benefit greatest in FLAIL CHEST - e.g. roughly 4% vs 10% mortality versus non-operative management), fewer pulmonary complications, more ventilator-free days and shorter ICU stays, at the cost of increased resource use.
- TIMING matters: EARLY SSRF (within roughly the first three days / ~82 hours) is associated with lower rates of ARDS and ventilator-associated pneumonia and shorter hospital stays than delayed fixation; benefit also extends beyond classic flail chest to selected patients with multiple displaced rib fractures, particularly those ventilated or with three or more fractures.
- The ORTHOPAEDIC relevance is direct: the orthopaedic/trauma surgeon may perform or assist with rib fixation, must recognise and manage ASSOCIATED skeletal injuries (scapula, clavicle, sternum, spine) and intrathoracic/abdominal injuries that accompany high-energy chest trauma, and must integrate chest-wall stabilisation into the overall polytrauma plan (including the timing of other orthopaedic procedures).
- “Flail chest = >=3 contiguous ribs each fractured in >=2 places -> paradoxical flail segment (high-energy injury).
- “Morbidity driven by PULMONARY CONTUSION + PAIN-related hypoventilation, NOT the paradox alone - priorities are oxygenation, multimodal/REGIONAL analgesia, pulmonary toilet, ventilatory support.
- “SSRF (rib fixation) lowers mortality/pulmonary complications - benefit greatest in FLAIL CHEST and when EARLY (~within 3 days). Look for associated scapula/clavicle/sternum/spine and intrathoracic injuries.
Flail chest = >=3 contiguous ribs fractured in >=2 places -> paradoxical segment. High-energy; look for associated scapula/clavicle/sternum/spine and intrathoracic injuries.
Morbidity is from pulmonary contusion + pain-related hypoventilation - prioritise oxygenation, multimodal/regional analgesia, pulmonary toilet. SSRF (early) improves outcomes.
Definition, Physiology & Management
Flail chest is three or more contiguous ribs each fractured in two or more places, creating a free segment that moves paradoxically (in on inspiration, out on expiration) - a high-energy injury. The morbidity, though, is driven mainly by the underlying pulmonary contusion and by pain-related hypoventilation (atelectasis, retained secretions, pneumonia, respiratory failure), NOT by the paradox alone. Management follows ATLS and centres on multimodal analgesia - including regional techniques (thoracic epidural, paravertebral, intercostal/erector-spinae blocks) - aggressive pulmonary toilet/physiotherapy, oxygen, and ventilatory support as needed. Surgical stabilisation of rib fractures (SSRF) is increasingly used and improves outcomes - lower mortality and pulmonary complications, more ventilator-free days - especially when performed early in flail chest. Look for associated skeletal (scapula, clavicle, sternum, spine) and intrathoracic/abdominal injuries.
- SSRF (rib fixation)
- Lower (~4%)
- Non-operative
- Higher (~10%)
- SSRF (rib fixation)
- Fewer complications, more ventilator-free days
- Non-operative
- More complications
- SSRF (rib fixation)
- Variable (can be longer stay/more resource)
- Non-operative
- -
- SSRF (rib fixation)
- Early (within ~3 days/82h) lowers ARDS/VAP
- Non-operative
- -
SSRF, Timing & Orthopaedic Role
- Analgesia and pulmonary care first/always: multimodal analgesia with regional techniques to enable deep breathing and coughing, aggressive pulmonary toilet/physiotherapy, oxygen, and escalation to non-invasive or invasive ventilation for respiratory failure.
- SSRF (rib plating) for flail chest and selected multiple displaced rib fractures: improves mortality and pulmonary outcomes; benefit greatest in flail chest and in ventilated patients / those with three or more fractures.
- Operate early: early SSRF (within ~3 days / ~82 hours) is associated with lower ARDS and ventilator-associated pneumonia and shorter stays than delayed fixation.
- The orthopaedic role: perform/assist rib fixation, recognise and manage associated skeletal injuries (scapula, clavicle, sternum, spine) and intrathoracic/abdominal injuries, and integrate chest-wall stabilisation into the polytrauma plan and the timing of other procedures.
Choosing the analgesic technique, not just listing them
Naming four regional options is not an answer; the examiner wants to know which and why, and what stops you.
- Thoracic epidural is the historic reference standard for multiple rib fractures and flail chest, giving bilateral segmental block and the best-documented improvement in pulmonary function. Its problem in this population is that it is frequently unavailable in practice: it is contraindicated or unwise with coagulopathy or therapeutic anticoagulation, haemodynamic instability (the sympathectomy will not be tolerated in a patient who is still bleeding), spinal fracture or spinal cord injury, and sepsis - all of which are common in exactly the polytrauma patient who has a flail chest.
- Paravertebral block gives comparable unilateral analgesia with less hypotension and urinary retention and is more tolerant of anticoagulation, making it a practical alternative when the epidural is contraindicated and the injury is one-sided.
- Erector spinae plane and serratus anterior plane blocks are superficial fascial-plane techniques that are far from the neuraxis, quick, ultrasound-guided and comparatively safe in the anticoagulated patient. They have largely displaced the older options in many units for this reason, and can be run as catheters.
- Intercostal blocks are simple but short-lived and multiple-injection, with the highest local anaesthetic absorption of the options, so they are best as a bridge.
- Systemic multimodal therapy underpins everything: regular paracetamol, NSAIDs where renal function and bleeding risk permit, and opioid by patient-controlled analgesia, with ketamine as an opioid-sparing adjunct. The goal is not comfort at rest but the ability to take a deep breath, cough and be sat out - analgesia should be titrated against incentive spirometry and the ability to clear secretions, not a pain score alone.
What the rib fixation operation actually involves
Having decided to stabilise the chest wall, the viva will ask how it is actually done.
- Positioning and approach follow the fracture location, guided by the CT with 3D reconstruction: posterolateral fractures through a lateral or posterolateral approach with the patient in the lateral position, anterior fractures anteriorly. Muscle-sparing approaches and windows between latissimus dorsi and serratus anterior limit morbidity.
- You do not fix every fracture. The aim is to restore the stability and contour of the chest wall, which usually means fixing the ends of the flail segment and the most displaced ribs - commonly ribs 4 to 9, since the first two are inaccessible beneath the scapula and clavicle and the floating ribs contribute little to stability.
- Implants are anatomically pre-contoured locking plates applied to the outer cortex, or intramedullary splints/rods for selected fractures where soft-tissue stripping is undesirable. Ribs are thin, so locking screws and adequate screw purchase matter, and the plate is positioned respecting the inferior-border neurovascular bundle.
- Thoracoscopy (VATS) is often used alongside to evacuate a retained haemothorax, confirm the reduction from inside, and assess for lung injury or a diaphragmatic tear.
- A chest drain is usually placed, and the pleura is inspected - an unrecognised pleural breach with positive-pressure ventilation is the immediate hazard.
- Specific complications: implant failure or migration, symptomatic hardware requiring removal, surgical site infection and empyema, pleural injury and pneumothorax, intercostal neuralgia, and nonunion. These are the counterbalance to the outcome benefits quoted above and belong in the consent discussion.
The classic error in flail chest is to focus on the dramatic paradoxical chest-wall motion while under-treating the things that actually cause death: the underlying pulmonary contusion and the pain-related hypoventilation that lead to atelectasis, pneumonia and respiratory failure. So the priorities are oxygenation, excellent multimodal analgesia (using regional techniques such as a thoracic epidural or paravertebral/erector-spinae blocks so the patient can breathe deeply and cough), aggressive pulmonary toilet, and timely escalation of respiratory support - with surgical stabilisation of rib fractures considered, especially early, in flail chest and selected multiple-rib-fracture patients to reduce mortality and pulmonary complications. As the orthopaedic member of the trauma team, also actively look for the associated scapula, clavicle, sternum and spine injuries and the intrathoracic and abdominal injuries that accompany this high-energy mechanism.
Which Ribs Are Broken Tells You What Else to Look For
The rib cage is a series of levers, and the pattern of fractures is a readable record of the energy and its direction - which is why the fracture level, not just the count, changes what you go looking for.
- Ribs 1 and 2 are short, thick and protected beneath the clavicle and scapula. Fracturing them takes very high energy, so they are a red flag for injury to the great vessels (subclavian and aortic), the brachial plexus, and the head, neck and spine. A first-rib fracture on a trauma film should prompt vascular assessment rather than reassurance.
- Ribs 3 to 10 are the ones that flail. They are the mobile, spring-loaded ribs, and the usual flail segment lies anterolaterally or laterally, where the ribs are longest and least supported.
- Ribs 9 to 12 are short, mobile and overlie the upper abdomen. Fractures here should raise liver, splenic and renal injury - a left lower rib fracture is a splenic injury until imaging says otherwise.
- The costal cartilages are radiolucent, so costochondral separations and cartilage injuries are invisible on plain film and are a recognised cause of an "occult" flail chest that is obvious clinically but unexplained radiographically. CT with 3D reconstruction resolves this.
The neurovascular bundle runs in the costal groove under the inferior border of each rib, in the order vein-artery-nerve from above down. Two practical consequences follow, and both are examinable: an intercostal block or a chest drain is placed over the superior border of the rib below to avoid the bundle, and during rib fixation the plate and screws are positioned with the bundle in mind, since an errant drill causes bleeding that is awkward to control and an intercostal neuralgia that is permanent.
Rib Fractures in the Elderly: The Numbers That Change Management
The single most examinable statistic in chest-wall trauma is not about flail chest at all - it is about how badly older patients tolerate any rib fracture.
According to the classic cohort, elderly patients (65 and over) sustaining rib fractures have roughly twice the mortality and thoracic morbidity of younger patients with comparable injuries - 22% versus 10% mortality, and 31% versus 17% pneumonia - despite similar fracture numbers and injury severity scores. And the risk scales with the count: each additional rib fracture increases mortality by about 19% and the risk of pneumonia by about 27%.
The practical consequences are what an examiner is after:
- An older patient with two or three rib fractures is not a minor injury to be discharged from the emergency department with codeine. That is the trap.
- Lower the threshold for admission, monitoring and aggressive analgesia in this group, and consider high-dependency care where the fracture count is high or the reserve poor.
- Count the fractures deliberately on CT and use the number as a risk score, not just a description.
- Institutional rib fracture pathways - protocolised analgesia, incentive spirometry, early physiotherapy and escalation criteria - exist precisely because this population deteriorates quietly at 48 to 72 hours.
Pulmonary Contusion: The Injury That Blossoms
The morbidity of a flail chest comes from the pulmonary contusion, and it is worth being precise about what that means. A contusion is a bruise of the lung parenchyma beneath the fractured segment: the impact ruptures alveolar capillaries so the alveoli fill with blood and oedema fluid, and surfactant is disrupted. The flooded, collapsed alveoli are still perfused but no longer ventilated, producing ventilation-perfusion mismatch and shunt - and therefore hypoxaemia out of proportion to the visible chest-wall injury.
The dangerous feature is its time course: the contusion "blossoms". It is frequently under-called on the initial chest radiograph and characteristically worsens, radiographically and physiologically, over the first 24 to 72 hours before slowly resolving over days to weeks. CT is far more sensitive than plain film and shows the true extent early; a large contused lung volume predicts ARDS and the need for ventilation. This delayed blossoming is exactly why a flail-chest patient can look stable on arrival and then deteriorate at 24 to 48 hours - so serial respiratory assessment, a low threshold for CT, and early escalation of support matter.
It also creates a fluid paradox: the contused lung is leaky, so over-resuscitation with crystalloid worsens the oedema and the contusion, yet the polytrauma patient may genuinely need volume for haemorrhage. The aim is therefore judicious, goal-directed fluid management - restore euvolaemia and treat shock, but avoid fluid overload - together with lung-protective ventilation if the patient is ventilated. (The overall resuscitation and damage-control framework belongs to Polytrauma Management and Damage Control Orthopaedics; the point here is the contusion-specific physiology this topic depends on.)
Pulmonary contusion = parenchymal bruise causing shunt and hypoxaemia; it blossoms over 24 to 72 hours, is often missed on the first radiograph (CT is more sensitive), and a large volume predicts ARDS. Over- resuscitation makes it worse - aim for euvolaemia, not fluid overload.
The Immediate Chest Killers to Exclude First
This is "a chest injury in a trauma patient", so before attention turns to the flail segment or SSRF the primary survey must exclude the immediately life-threatening thoracic injuries - high-energy rib fractures frequently cause them:
- Tension pneumothorax - air trapped under pressure with mediastinal shift: respiratory distress, hypotension, distended neck veins, tracheal deviation away from the side, absent breath sounds with hyperresonance. It is a clinical diagnosis treated immediately by needle or finger decompression and then a chest drain - do not wait for a radiograph.
- Open pneumothorax (a "sucking" chest-wall wound) - cover with a dressing taped on three sides (a flutter valve) and then place a chest drain away from the wound.
- Massive haemothorax - large blood loss into the hemithorax: absent breath sounds with dullness and shock; treat with a chest drain plus blood/volume, and thoracotomy for a large immediate or ongoing output.
- Cardiac tamponade - Beck's triad (hypotension, muffled heart sounds, raised JVP), diagnosed on FAST; needs pericardial drainage or surgery.
Flail chest itself is one of the breathing problems on this list. The practical message: if a flail-chest patient deteriorates, exclude a (tension) pneumothorax or haemothorax first - and remember that starting positive-pressure ventilation can convert a simple pneumothorax into a tension pneumothorax.
In chest-wall trauma, clear the immediate killers first: tension pneumothorax (clinical diagnosis, immediate decompression), open pneumothorax (three-sided dressing), massive haemothorax (drain plus blood, thoracotomy if high output), cardiac tamponade (Beck's triad, FAST). Rib fixation comes after the primary survey - and beware tensioning a simple pneumothorax once you ventilate.
Complications and What Happens Afterwards
The acute phase dominates the teaching, but flail chest is not an injury people simply recover from, and the long-term picture is a fair viva question.
In hospital, the complications follow directly from the physiology above: pneumonia is the commonest, along with atelectasis and retained secretions, ARDS where the contusion is large, prolonged ventilation and its consequences including tracheostomy, retained haemothorax and empyema, and pneumothorax - which can appear late and can be tensioned by positive-pressure ventilation.
Afterwards, three things are consistently under-appreciated:
- Chronic chest wall pain is common and can persist for a year or more, sometimes as a neuropathic intercostal neuralgia rather than as fracture pain, and it responds poorly to opioids.
- Persistent disability and delayed return to work are the rule rather than the exception after a flail chest, with reduced exercise tolerance and measurable restrictive impairment on lung function testing in a substantial minority.
- Symptomatic nonunion and chest wall deformity occur, and are one of the accepted later indications for rib fixation in a patient who was managed non-operatively at the time.
Because of this, follow-up should be active rather than assumed: review pain and function, screen for the neuropathic component, and involve pain services and rehabilitation early rather than treating a healed radiograph as the end of the episode.
Mnemonics & Memory Aids
FLAIL
Hook:FLAIL: Free segment, Lung contusion (the real problem), Analgesia+pulmonary toilet, Involved associated injuries, Lock the ribs (early SSRF).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is flail chest, and why does it cause respiratory compromise?”
“What is the role of surgical stabilisation of rib fractures, and when would you operate?”
Definition
- >=3 contiguous ribs each fractured in >=2 places -> free flail segment
- Paradoxical motion (in on inspiration, out on expiration)
- Marker of high-energy chest trauma
Why it harms
- Pulmonary contusion impairs gas exchange
- Pain-related splinting/hypoventilation -> atelectasis, pneumonia, respiratory failure
- NOT the paradox alone
Management
- ATLS; oxygenation; multimodal analgesia incl. regional (epidural/paravertebral/erector-spinae)
- Aggressive pulmonary toilet/physiotherapy; non-invasive/invasive ventilation as needed
- Look for associated scapula/clavicle/sternum/spine + intrathoracic/abdominal injuries
SSRF
- Rib plating improves mortality/pulmonary outcomes - benefit greatest in flail chest
- Also benefits selected multiple displaced rib fractures (ventilated / >=3 fractures)
- Operate early (within ~3 days/82h) - lower ARDS/VAP, shorter stay
Evidence & Key Studies
Early surgical stabilisation of multiple rib fractures and flail chest vs nonoperative management
- In a nationwide analysis (3,806 SSRF vs weighted controls) of adults with three or more rib fractures, surgical stabilisation was associated with lower in-hospital mortality (1.5% vs 2.7%), with the benefit greatest in flail chest (4.2% vs 10.1%).
- SSRF was associated with longer hospital and ICU stays (increased resource use).
- Early SSRF (within ~82 hours) had similar mortality to delayed fixation but lower rates of ARDS and ventilator-associated pneumonia and shorter hospital stays.
Real-world impact of surgical stabilisation of rib fractures beyond flail chest
- Surgical stabilisation of rib fractures (SSRF) improved outcomes beyond classic flail chest, benefiting patients with multiple rib fractures with and without mechanical ventilation.
- SSRF patients had significantly longer ventilator-free days at day 28 and a trend to reduced non-procedural pulmonary complications.
- Patients not ventilated but with more than three rib fractures also benefited from SSRF, supporting broader application.
Rib fractures in the elderly
- 277 patients aged 65 or over with rib fractures compared with 187 patients aged 18-64, matched closely for mean number of fractures (3.6 vs 4.0), chest AIS (3.0 vs 3.0) and ISS (20.7 vs 21.4).
- Despite comparable injuries, the elderly had double the harm: mortality 22% versus 10% and pneumonia 31% versus 17%, with longer ventilator, ICU and hospital stays.
- Risk scaled with fracture count - for each additional rib fracture in the elderly, mortality increased by 19% and the risk of pneumonia by 27%.
The survival benefit of surgical stabilisation of rib fractures (with the greatest benefit in flail chest), the increased resource use, and the advantage of early (within ~82 hours) fixation in reducing ARDS and ventilator-associated pneumonia come from the cited Kwon nationwide analysis; the benefit of SSRF beyond classic flail chest (more ventilator-free days, fewer pulmonary complications, including in non-ventilated patients with more than three fractures) from the cited Tang study. The definition of flail chest, the primacy of pulmonary contusion and pain-related hypoventilation, the multimodal/regional analgesia and pulmonary-toilet management, and the associated-injury considerations are standard, well-established teaching. The elderly rib-fracture mortality and pneumonia figures, and the 19%/27% increase per additional fracture, come from the cited Bulger cohort. The rib-level anatomy, the choice between regional techniques and their contraindications, the operative technique of rib fixation and its specific complications, and the long-term outcomes are standard trauma teaching. (See also Polytrauma Management, Damage Control Orthopaedics, ATLS Primary Survey, Scapula Fractures and Clavicle Fractures.)