Inferior Glenohumeral Dislocation
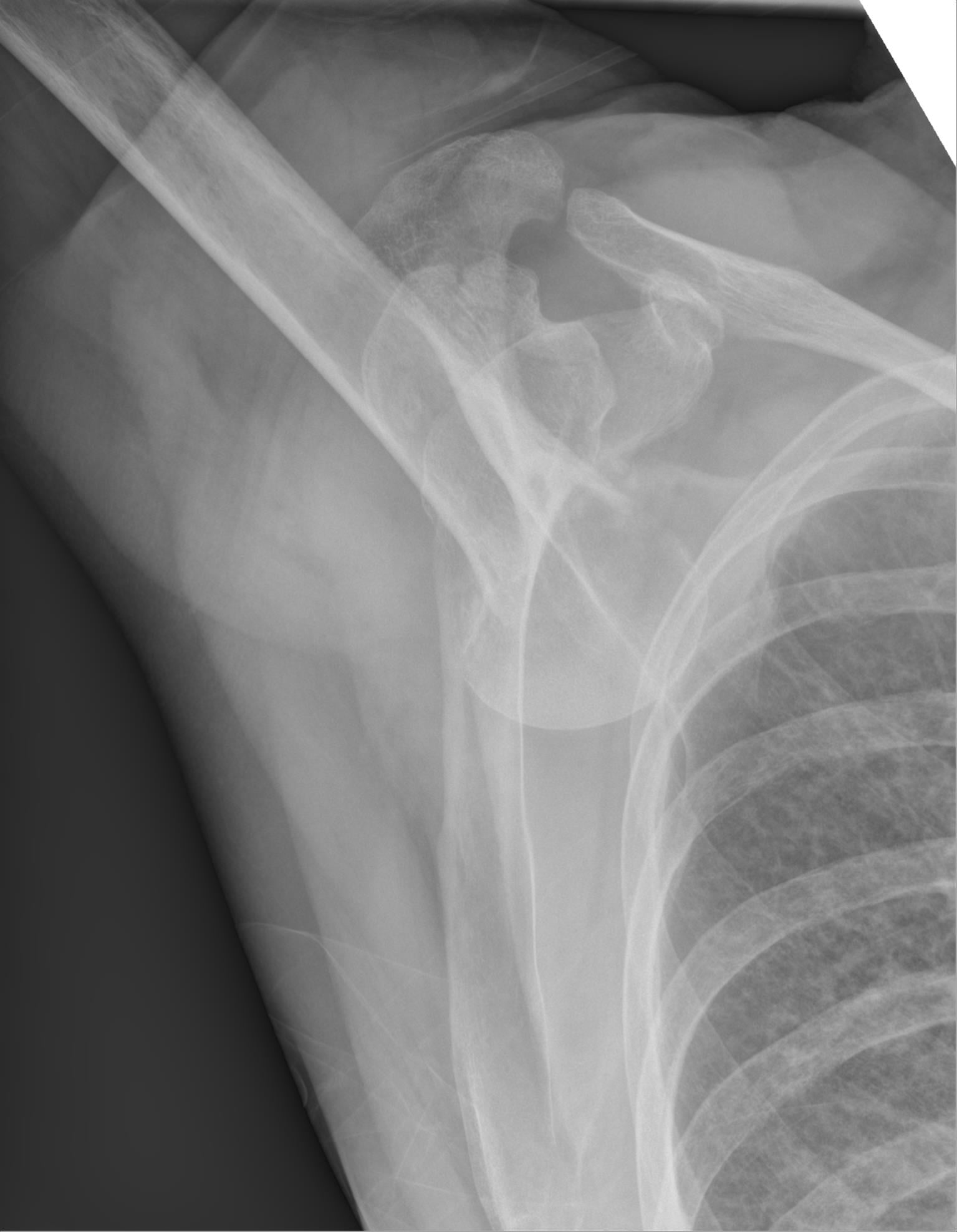
- Luxatio erecta humeri is an INFERIOR glenohumeral dislocation - the humeral head lies below the glenoid and the arm is locked RIGIDLY HYPERABDUCTED above the head, a position the patient cannot reverse; it is the rarest type of shoulder dislocation (under 1%) and the diagnosis is a 'spot diagnosis' on the clinical picture and AP radiograph (the abducted humeral shaft points superolaterally with the head inferior to the glenoid).
- The mechanism is either a direct AXIAL LOAD applied to a fully abducted extremity, or a HYPERABDUCTION force that levers the humeral head inferiorly across the acromion - the two recognised pathomechanics.
- There is a HIGH incidence of NEUROVASCULAR injury: brachial plexus and axillary nerve neuropraxia (and radial/ulnar involvement) and axillary ARTERY injury (intimal tear, transection or thrombosis) or venous injury - so a careful neurovascular examination MUST be documented before and after reduction, and vascular compromise requires urgent assessment.
- Associated MUSCULOSKELETAL injuries are common: ROTATOR-CUFF tears, greater-tuberosity avulsion, and impaction defects of the humeral head (and fractures of the acromion, clavicle or coracoid) - the cuff injury in particular drives later morbidity, so the cuff should be assessed after reduction.
- Closed reduction is by TRACTION-COUNTERTRACTION: axial traction along the abducted arm with countertraction over the shoulder, gradually bringing the arm into adduction (a 'two-step' technique converts it to an anterior-type position then reduces); it is usually achieved under sedation/analgesia, with rare cases (button-holing of the head through the capsule) needing open reduction.
- After reduction the arm is immobilised in a sling in ADDUCTION, neurovascular status and the rotator cuff are re-checked, and follow-up addresses the high rates of recurrent instability, residual cuff dysfunction and adhesive capsulitis; orthopaedic referral is warranted because of the frequent cuff injury.
- “Luxatio erecta = INFERIOR dislocation: arm LOCKED hyperabducted ABOVE the head (cannot bring it down) - unmistakable spot diagnosis.
- “HIGH neurovascular risk (brachial plexus/axillary nerve, axillary artery) + rotator-cuff/greater-tuberosity injury - examine before AND after reduction.
- “Reduce by TRACTION-COUNTERTRACTION (or two-step) under sedation, then sling in adduction; rare button-hole cases need open reduction.
Arm locked hyperabducted above the head, elbow flexed, forearm resting on or behind the head - the patient cannot bring it down. The head is palpable on the lateral chest wall.
Neurovascular injury (brachial plexus / axillary artery) and rotator-cuff / greater-tuberosity damage are common - examine and document before and after reduction.
Mechanism, Recognition & Associated Injury
Luxatio erecta is the inferior glenohumeral dislocation - the rarest type (under 1% of shoulder dislocations) - and is produced either by an axial load on a fully abducted arm or by a hyperabduction force that levers the humeral head inferiorly over the acromion. The presentation is unmistakable: the arm is held rigidly hyperabducted above the head and cannot be brought down, with the head palpable on the lateral chest wall. Despite the dramatic, easy picture, the company it keeps is dangerous - there is a high incidence of brachial plexus / axillary nerve neuropraxia, axillary artery injury (intimal tear, transection or thrombosis), and rotator-cuff tears with greater-tuberosity avulsion and humeral-head impaction. It is frequently misdiagnosed as an anterior dislocation if the classic position is not appreciated.
What Is Actually Torn and Broken: the Cross-Sectional Imaging Picture
"A high rate of associated injury" is repeated about this dislocation more often than it is quantified. The one series that examined every case with CT and/or MRI rather than radiographs found the following in 10 shoulders - a small number, and the reason each figure below is given as a count rather than a percentage:
- Number of the 10
- 6
- Why it matters
- The commonest single finding - and the one that changes management, since a displaced tuberosity is a surgical indication in its own right
- Number of the 10
- 4
- Why it matters
- A bony Bankart equivalent; relevant to later instability and often invisible on the trauma AP
- Number of the 10
- 4
- Why it matters
- The inferior-dislocation analogue of a Hill-Sachs lesion
- Number of the 10
- 4
- Why it matters
- Torn twice as often as the cuff in this series
- Number of the 10
- 2
- Why it matters
- Real, but not the dominant lesion that the classic teaching implies
- Number of the 10
- 2
- Why it matters
- The structure through which the head escapes - the pathoanatomy made visible
- Number of the 10
- 2
- Why it matters
- A driver of late symptoms independent of instability
Two things follow. First, the injury is predominantly bony and labral, not simply a cuff injury. The long-standing teaching that a rotator-cuff tear is the defining associated lesion comes from clinical and radiographic series in older cohorts, and remains true of the elderly patient - but a young patient with this injury is more likely to have a glenoid rim fracture, an impaction defect and a labral tear, which is a different problem with a different follow-up. Second, plain radiographs will under-report all of it, which is the practical argument for post-reduction CT where there is any suggestion of a fracture, and MRI where the cuff or labrum is in question - not as a routine reflex, but because the injuries that determine outcome are the ones the trauma films are worst at showing.
Age remains the most useful single guide to what to expect and therefore what to image: over roughly 40, the question is the cuff; under 40, the question is the labrum, the glenoid rim and later instability.
What 'Examine the Neurovascular Status' Actually Means Here
An instruction to examine and document the neurovascular status is worth nothing without the examination itself, and this is a shoulder that cannot be adducted, in a patient in severe pain, so the examination has to be chosen to be feasible in that position.
The nerves. Involvement is usually a traction neurapraxia of the infraclavicular brachial plexus rather than an isolated axillary nerve palsy, so testing the axillary nerve alone will miss most of it. Test and record, by nerve:
- Motor test that works with the arm still up
- Palpate the deltoid for contraction as the patient attempts to push the arm further into abduction - do NOT ask for abduction against gravity from a reduced position, which is impossible here
- Sensory
- Regimental badge patch over the lateral deltoid
- Motor test that works with the arm still up
- Elbow flexion with the forearm supinated; palpate biceps
- Sensory
- Lateral forearm
- Motor test that works with the arm still up
- Wrist and finger extension, thumb extension
- Sensory
- First dorsal web space
- Motor test that works with the arm still up
- Thumb opposition / abductor pollicis brevis
- Sensory
- Volar index fingertip
- Motor test that works with the arm still up
- Finger abduction (first dorsal interosseous), crossing fingers
- Sensory
- Volar little fingertip
Record this before analgesia and sedation as well as after reduction, because a deficit found only afterwards cannot be attributed - and the distinction between a deficit caused by the injury and one caused by the reduction is precisely what will be asked, in the exam and later.
The vessel. A palpable radial pulse does not exclude an axillary artery injury: the collateral circulation around the scapula can maintain a pulse distal to an intimal tear or a partially thrombosed segment. The assessment is therefore graded rather than binary, and follows the same rule used elsewhere in limb trauma:
- What it means
- Arterial injury until proven otherwise
- What to do
- Vascular surgery immediately, and do not delay theatre for imaging when the limb is ischaemic
- What it means
- Possible injury; needs objective testing
- What to do
- Measure the arterial pressure index and image - CT angiography, or duplex where available and reliable
- What it means
- The accepted screening threshold for occult arterial injury
- What to do
- CT angiography
- What it means
- Screen negative
- What to do
- Serial re-examination - a delayed thrombosis can still declare itself over the following hours
The same threshold and sequence apply to limb vascular injury generally, set out in Vascular Injury in Fracture-Dislocation - so 0.9 is one number that carries across every dislocation and fracture with a limb at risk.
A displaced proximal humeral fracture - typically a valgus-impacted or surgical-neck fracture in an elderly osteoporotic patient - can leave the arm apparently fixed in abduction and produce a radiograph in which the head sits low relative to the glenoid, mimicking an inferior dislocation. It is not one: the head remains located, and the deformity is at the fracture, not the joint.
Why it matters more than a naming point. Traction-countertraction applied to a fracture achieves nothing, displaces the fragments further, and can convert a fracture that would have been managed in a sling into one needing fixation, with a devitalised head. Look at the glenoid before you pull. In a true luxatio erecta the glenoid fossa is EMPTY and the articular surface of the head faces inferiorly; in a fracture-dislocation mimic the head remains congruent with the glenoid while the shaft is displaced. If the radiograph is not unambiguous, get a CT before any reduction attempt - and remember that a genuine inferior dislocation can also carry a displaced greater tuberosity or surgical-neck fracture, in which case traction risks completing it. (See Proximal Humerus Fractures.)
Reduction in Detail: Traction-Countertraction, the Two-Step, and When It Will Not Reduce
Traction-countertraction, the two-step technique and open reduction for a button-holed head are each described below, because the steps themselves are what the examiner asks for at the bedside.
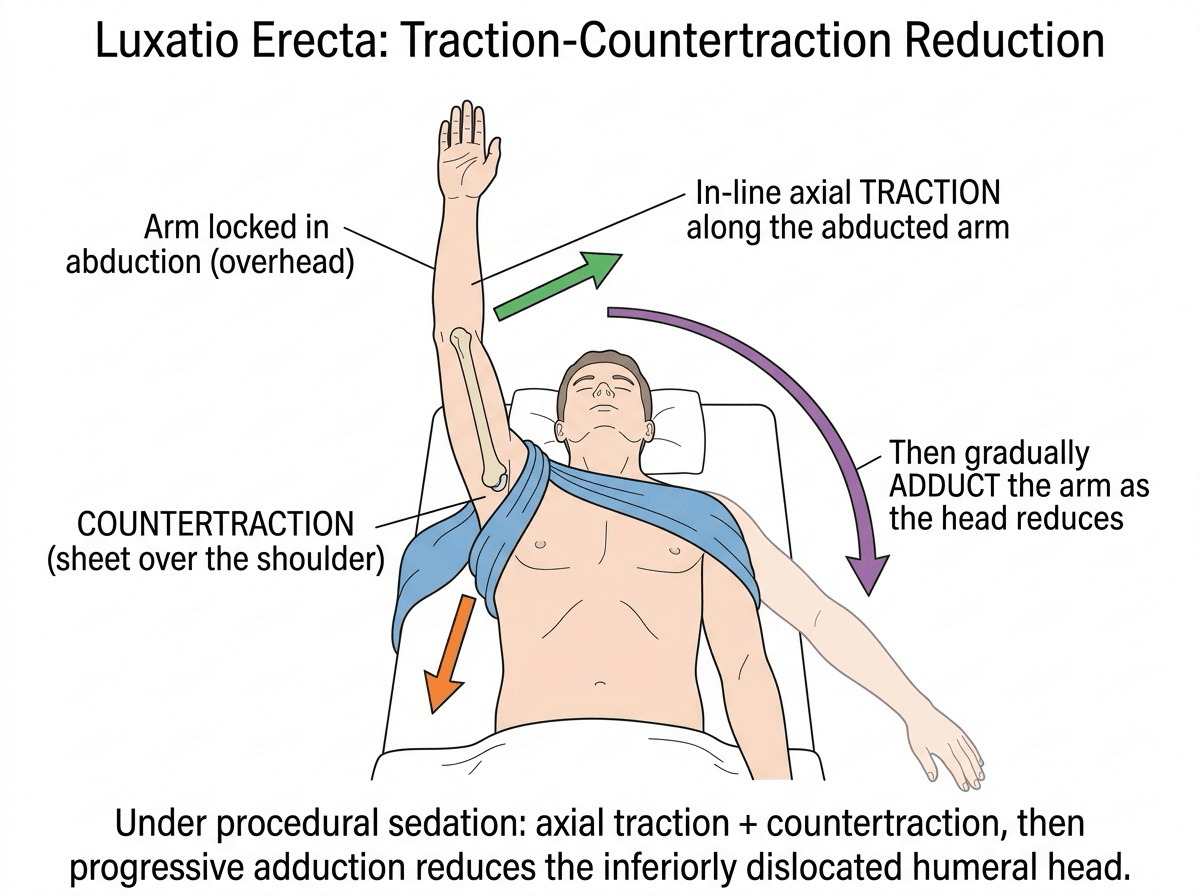
- Traction-countertraction: in-line axial traction along the abducted humerus with countertraction by a sheet across the shoulder/over the trapezius; gradually adduct the arm as the head reduces. Under procedural sedation/analgesia.
- Two-step technique: Step 1 - convert the inferior (subglenoid) dislocation into an anterior one by pushing the humeral head anteriorly while gently adducting; Step 2 - reduce the resulting anterior dislocation by a standard manoeuvre. Useful when straight traction-countertraction fails; a single-operator variant exists.
Suspect an irreducible dislocation when the head is button-holed through an inferior capsular rent, or when the cuff, the long head of biceps or a bone fragment is interposed (or the head is buttonholed around the glenoid neck) - these block closed reduction and need open reduction. Displaced associated fractures may also require fixation.
Closed reduction is traction-countertraction with progressive adduction, or the two-step (convert to an anterior dislocation, then reduce it). If it will not go, suspect a button-holed head or interposed tissue and proceed to open reduction - then sling in adduction and re-check nerves, pulse and cuff.
After reduction: a workable schedule
Repeat the full nerve-by-nerve examination and the pulse assessment, and obtain orthogonal post-reduction radiographs - an AP and an axillary or modified axillary view, because concentric reduction cannot be judged on a single projection. Look specifically for a greater tuberosity fragment that has become displaced during the manoeuvre.
Immobilise for two to three weeks - long enough for the inferior capsular rent to begin healing, short enough to avoid a stiff shoulder, which in this injury is a greater practical risk than recurrent instability. Elbow, wrist and hand movement from the first day; pendulum exercises within comfort.
Arrange CT if any fracture is suspected and MRI if cuff or labral injury is suspected on the grounds above. In a patient over about 40 who cannot initiate abduction once the pain has settled, distinguish a cuff tear from a persisting axillary neurapraxia - the histories overlap and the treatments do not.
Progressive active-assisted then active range of motion, avoiding forced abduction and external rotation at the extremes early. Adhesive capsulitis is a recognised outcome of this injury and is prevented by movement, not by rest.
Rotator-cuff and scapular strengthening. Review the neurological deficit: most traction neurapraxias recover over weeks to a few months, and failure to show clinical or electrophysiological recovery by around three months is the point to obtain nerve conduction studies and EMG and to consider a brachial plexus opinion rather than continuing to wait.
Pathoanatomy: Why the Arm Locks Overhead
The head button-holed through a capsular rent, levering over the acromion, and cuff or tuberosity avulsion are all consequences of one pathoanatomy - and it is that pathoanatomy which ties the locked position to the dangerous associations.
The humeral head is driven inferiorly through a tear in the inferior capsule and comes to lie below the glenoid (subglenoid), while the humeral shaft/surgical neck levers against and abuts the acromion (and the lateral scapula). This mechanical block holds the arm rigidly hyperabducted overhead - which is why the patient cannot adduct it, and why a head button-holed through the capsule may be irreducible closed.
The same displacement avulses the superior structures - the rotator cuff, the greater tuberosity, with humeral-head impaction - explaining the high cuff/tuberosity injury rate. And the inferiorly displaced head stretches and compresses the axillary neurovascular bundle in the axilla - the anatomical basis for the high rate of brachial plexus/axillary nerve and axillary artery injury.
The head buttonholes inferiorly through the inferior capsule and the shaft levers on the acromion (the block that locks the arm up); the superior cuff/greater tuberosity is avulsed and the axillary neurovascular bundle stretched - one pathoanatomy that explains both the position and the associations.
Reduction & Aftercare
- Assess first: document neurovascular status (brachial plexus, axillary nerve, distal pulses/perfusion) - and re-check after reduction.
- Closed reduction (traction-countertraction): apply axial traction along the line of the abducted humerus with countertraction across the shoulder (a sheet over the shoulder), and gradually swing the arm into adduction to relocate the head. Performed under sedation/analgesia.
- Two-step technique: convert the inferior dislocation to an anterior-type position and then reduce - useful when straight traction-countertraction is difficult.
- Open reduction is reserved for the irreducible case (e.g. the head 'button-holed' through a capsular rent) or for associated injuries requiring fixation.
- After reduction: immobilise in a sling in adduction, confirm relocation and neurovascular status radiographically/clinically, and assess the rotator cuff - referral is warranted because of the high rate of cuff injury.
The single most important habit in luxatio erecta is a documented neurovascular examination BEFORE and AFTER reduction, because the brachial plexus / axillary nerve and the axillary artery are frequently injured by the inferiorly displaced head, and a vascular injury (intimal tear, thrombosis or transection) can be limb- threatening and is easy to overlook in the drama of the obvious deformity. After relocation, re-examine the nerves and the pulse and assess the rotator cuff, since an unrecognised cuff tear or arterial injury changes management. Treat luxatio erecta as a high-energy shoulder injury with dangerous associations, not merely as a striking position to be reduced.
Mnemonics & Memory Aids
ERECTA
Hook:ERECTA: arm Elevated, Rotator cuff torn, Examine nerves, check Circulation, Traction reduction, Adduction sling.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient arrives with the arm fixed above the head and cannot bring it down. What is the diagnosis and how do you manage it?”
“What associated injuries and complications would you specifically look for after reducing a luxatio erecta?”
Recognition
- Inferior glenohumeral dislocation - rarest type (under 1%)
- Arm locked rigidly hyperabducted above the head; cannot adduct
- Head palpable on lateral chest wall; AP X-ray: head below glenoid, shaft superolateral
Mechanism
- Axial load on a fully abducted arm, OR
- Hyperabduction force levering the head inferiorly over the acromion
- Often misdiagnosed as anterior dislocation
Associated injury
- Neurovascular: brachial plexus/axillary nerve neuropraxia; axillary artery injury
- Rotator-cuff tear, greater-tuberosity avulsion, humeral-head impaction
- Fractures of acromion, clavicle, coracoid
Management
- Document neurovascular status before AND after reduction
- Traction-countertraction (or two-step) under sedation; sling in adduction
- Open reduction if button-holed/irreducible; orthopaedic follow-up for the cuff
Evidence & Key Studies
Luxatio erecta humeri (pathomechanics, neurovascular injury, reduction and morbidity)
- Pathomechanics involve either direct axial loading on a fully abducted extremity or leverage of the humeral head across the acromion by a hyperabduction force; the affected arm is held rigidly above the head in abduction.
- Reduction is by traction-countertraction under sedation and analgesia; a variety of neurologic (brachial plexus) and vascular (axillary artery) injuries may be associated, along with fractures of the acromion, clavicle, coracoid, greater tuberosity and humeral head.
- It is associated with significant late morbidity including recurrent dislocation, instability and adhesive capsulitis.
Luxatio erecta: a rarely seen, but often missed shoulder dislocation
- Luxatio erecta is often misdiagnosed as an anterior dislocation; the presentation is unmistakable - the arm hyperabducted and locked above the head.
- Neurovascular injuries include neuropraxia of the brachial plexus and radial/ulnar nerves, and axillary artery/vein injury (intimal tears, transection, thrombosis).
- Reduction is by the traction-countertraction manoeuvre, after which the arm is maintained in a sling in adduction; orthopaedic referral is required because of the high incidence of rotator-cuff injury.
CT and MRI manifestations of luxatio erecta humeri
- 10 cases of luxatio erecta studied with CT and/or MRI rather than radiographs alone.
- Bony injury dominated: 6 comminuted displaced greater tuberosity fractures, 4 anterior-inferior glenoid fractures and 4 humeral head impaction fractures.
- Soft-tissue injury: 4 labral tears, 2 rotator cuff tears, 2 inferior glenohumeral ligament tears and 2 glenohumeral cartilage defects - the labrum was torn twice as often as the cuff.
- Small series (n = 10), so the counts indicate the pattern of injury rather than reliable population rates.
The pathomechanics (axial load on an abducted arm or hyperabduction leverage over the acromion), the traction-countertraction reduction, the spectrum of neurovascular injury (brachial plexus / axillary nerve and axillary artery/vein) and associated fractures, and the late morbidity (recurrent instability, adhesive capsulitis) come from the cited Davids report; the frequent misdiagnosis as anterior dislocation, the radial/ulnar neuropraxia and the high rate of rotator-cuff injury from the cited Grate review. The structural injury profile on cross-sectional imaging - the six greater-tuberosity fractures, four glenoid fractures, four impaction fractures, four labral tears and two cuff tears in ten shoulders - comes from the cited Hassanzadeh series, whose small size is the reason those are given as counts. No reliable pooled percentage exists for the neurological or arterial injury rate in this dislocation; the literature is case reports and small series, which is precisely why every patient is examined rather than a defined at-risk group screened. The arterial pressure index threshold of 0.9 and the hard/soft-sign framework follow Vascular Injury in Fracture-Dislocation. The 'two-step' reduction technique and the immobilisation and rehabilitation schedule are standard, well-established teaching. (See also Anterior Shoulder Instability, Rotator Cuff Tears, Proximal Humerus Fractures and Axillary Nerve Anatomy.)