Fractures Around Shoulder and Elbow Replacements
- Periprosthetic fractures around SHOULDER and ELBOW arthroplasty are an increasingly common complication as these replacements become more frequent; they typically occur in ELDERLY, often OSTEOPOROTIC bone, and management is guided by the same logic as the hip: FRACTURE LOCATION, IMPLANT STABILITY and BONE QUALITY.
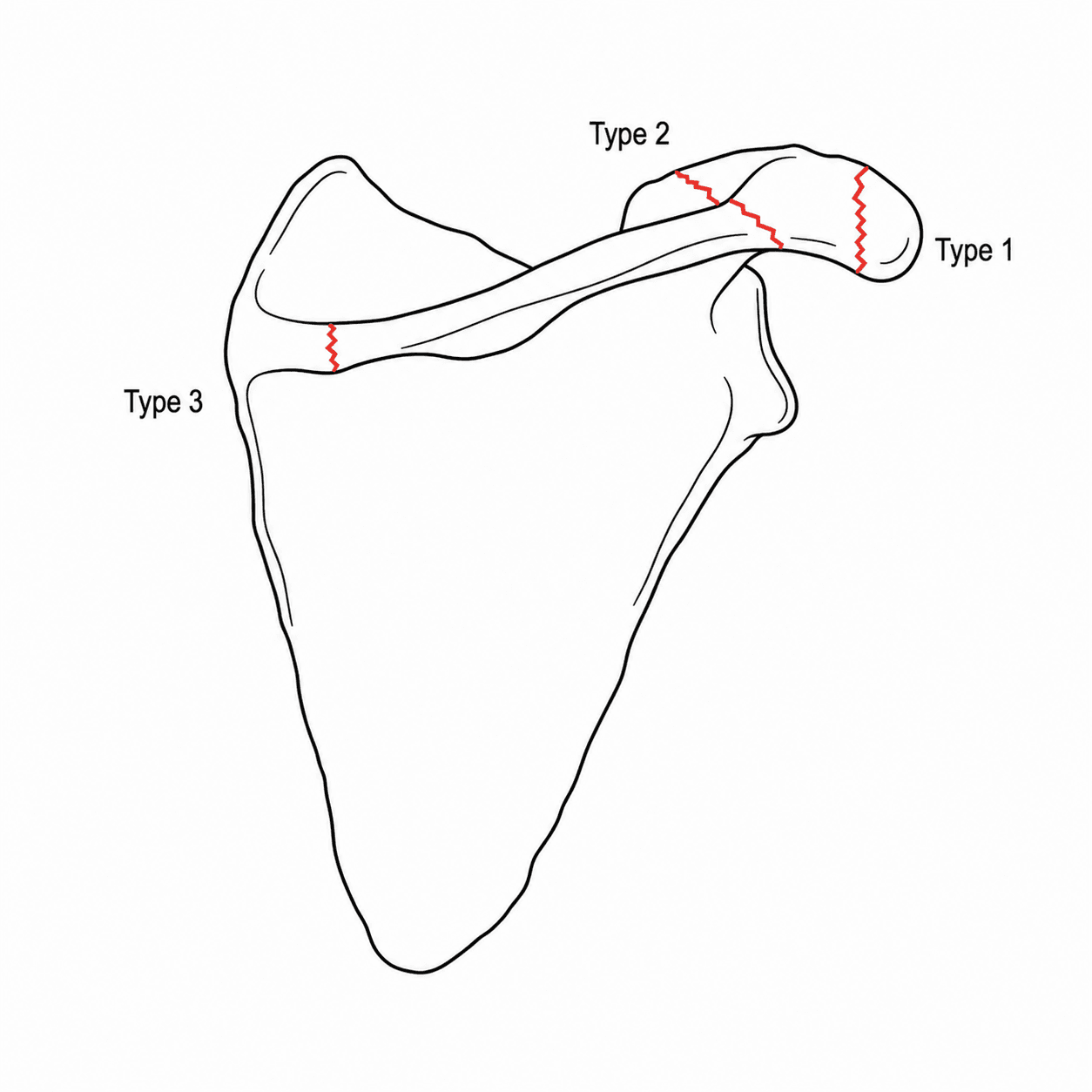
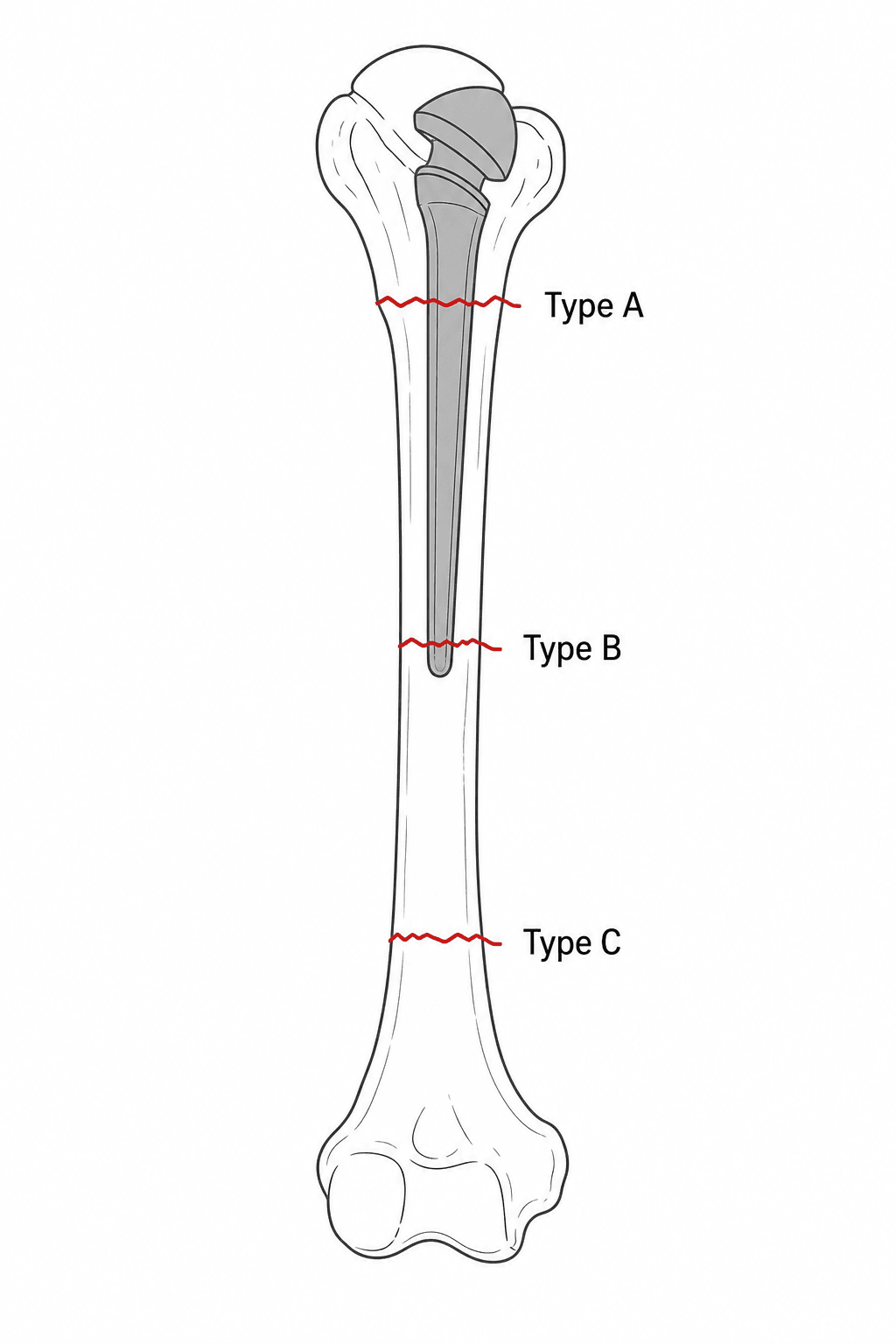
- For the SHOULDER (periprosthetic humeral fracture after anatomic or reverse arthroplasty), the location-based classifications describe the fracture RELATIVE TO THE STEM TIP - the WRIGHT & COFIELD system (Type A at/proximal to the tip, Type B around/just distal to the tip, Type C distal/diaphyseal) is the most commonly used and the most RELIABLE, although interobserver agreement across all the shoulder systems is only MODERATE.
- For the ELBOW (periprosthetic fracture after total elbow arthroplasty), the MAYO classification (O'Driscoll & Morrey) grades by location and stem fixation: Type I about the ARTICULATION/columns (condyles), Type II along the STEM (humeral or ulnar component, subdivided by whether the stem is WELL-FIXED or LOOSE), and Type III BEYOND the stem tip; the thin ulna and bone loss make these challenging.
- The TREATMENT PRINCIPLE (Vancouver-style) is: if the implant is WELL-FIXED, treat the fracture (ORIF with plates, cerclage and often a STRUT ALLOGRAFT, or non-operatively for stable proximal/undisplaced patterns); if the implant is LOOSE, REVISE the implant (a longer-stemmed component that bypasses the fracture) with or without additional fixation/graft.
- Because the bone is frequently OSTEOPOROTIC and stock is limited (especially in revision and around the elbow), fixation strategies emphasise LONG plates, MULTIPLE points of fixation, CERCLAGE around the stem, and STRUT ALLOGRAFT to augment the construct; healing rates are good with appropriate, stability-matched treatment.
- Assess the WHOLE construct and the patient: identify the implant type, determine stem fixation (loosening signs), evaluate bone quality and the fracture pattern on radiographs (+/- CT), and rule out INFECTION before any revision.
- “Shoulder periprosthetic humeral fracture: classify by location relative to the STEM TIP (Wright & Cofield A/B/C; the most reliable system).
- “Elbow periprosthetic fracture: Mayo (O'Driscoll-Morrey) - Type I condyles/articulation, Type II along the stem (well-fixed vs loose), Type III beyond the stem.
- “Same principle as the hip (Vancouver): well-fixed implant -> ORIF (+/- strut allograft); loose implant -> revise with a long-stem component.
Treat the fracture: ORIF with a long plate, cerclage and often a strut allograft, or non-operative management for stable, undisplaced or proximal patterns. Keep the well-functioning implant.
Revise the implant with a longer-stemmed component that bypasses the fracture, with or without supplementary fixation/graft - fixing the fracture alone over a loose stem will fail.
Classifications
- Location relative to the stem tip
- At / proximal to the stem tip, extending proximally (around tuberosities/proximal stem)
- Location relative to the stem tip
- Around or just distal to the stem tip
- Location relative to the stem tip
- Distal to the stem tip (distal humeral diaphysis)
- Location
- About the ARTICULATION / columns (condyles) - around the joint, not the stem
- Location
- Along the STEM (humeral or ulnar) - subdivided by whether the stem is well-fixed or loose
- Location
- BEYOND the stem tip (diaphyseal)
For the shoulder, multiple classification systems exist (Wright & Cofield, Campbell, Worland, Groh); the Wright & Cofield system has the best intra- and interobserver reliability, but agreement across all systems - and on the preferred treatment - is only MODERATE, so the classification guides, but does not replace, individualised assessment of stem fixation and bone quality.
Assessment & Management
- Identify the implant (anatomic vs reverse shoulder; linked vs unlinked elbow) and stem fixation (loosening: lucency, subsidence, cement-mantle failure)
- Radiographs (+/- CT) for fracture pattern and location relative to the stem tip
- Assess bone quality/stock; rule out INFECTION before any revision
- Neurovascular exam (e.g. radial nerve with humeral fractures)
- Well-fixed implant: treat the fracture - ORIF (long plate, cerclage, screws) often with a strut allograft; non-operative for selected stable/undisplaced patterns
- Loose implant: revise to a long-stem component bypassing the fracture (+/- fixation/graft)
- Augment the osteoporotic construct (long plates, multiple fixation points, cerclage, strut graft)
- Shoulder (humerus): a Type C (distal, well below a well-fixed stem) is usually ORIF like a humeral shaft fracture; a fracture around a loose stem needs revision with a long stem; strut allograft (e.g. via a posterior approach with a plate) is valuable in osteoporotic bone and for Worland B/C-type patterns. Protect the radial nerve.
- Elbow: Type II fractures hinge on stem fixation - a well-fixed stem allows ORIF, a loose stem needs component revision; the thin ulna and condylar bone loss make fixation difficult, and strut allograft / revision implants are often required.
- Always treat within overall patient optimisation (the typical patient is elderly with osteoporosis and comorbidities) and exclude infection.
Intra-operative Periprosthetic Fractures
- Shoulder: during humeral preparation (broaching/reaming and especially stem impaction of a press-fit/uncemented stem in osteoporotic or stiff/ankylosed shoulders); during forceful dislocation, reduction and arm manipulation/retraction (torque on a stiff arthritic or revision shoulder can spiral the humeral shaft); during glenoid exposure/reaming; and with cement pressurisation.
- Elbow: the thin ulna and deficient distal humeral columns crack during canal preparation, broaching and component impaction.
Recognise it on the table - a feel or sound of a crack, then inspect and image intra-operatively, because an unrecognised intra-operative fracture presents later as early post-operative pain, loss of fixation or loosening. Treat it immediately: cerclage cables around the fracture, a longer stem to bypass it, strut graft as needed, and protect/modify the rehabilitation. Prevent it with gentle technique, adequate soft-tissue releases and exposure before levering, careful sequential broaching, and heightened awareness in osteoporotic, revision and stiff cases.
Many periprosthetic shoulder/elbow fractures are intra-operative - at stem impaction/broaching, forceful dislocation/manipulation, glenoid reaming (shoulder), or thin-ulna/column preparation (elbow). Recognise on the table (feel/inspect/image), treat immediately with cerclage plus a longer bypassing stem plus graft, and prevent with releases and gentle broaching in fragile bone.
Preventing the Next One: the Bone, the Nerve and the Weight Limit
Osteoporotic bone is named repeatedly as the reason these fractures happen and are hard to fix, and it is then usually left there as an adjective. Three things follow from it that belong in the treatment plan rather than the description.
Treat the osteoporosis - a periprosthetic fracture is a fragility fracture. A low-energy fall that breaks a humerus around a stem is the same event as any other fragility fracture, and carries the same implication: this patient will have another. The fracture should trigger a bone-health assessment - falls assessment, vitamin D and calcium, DXA where it will change management, and consideration of anti-resorptive or anabolic therapy - exactly as a wrist or hip fragility fracture does. Fixing the humerus and discharging the patient treats the event and ignores the disease.
Know which nerve is at risk, because it differs by site. For the humerus it is the radial nerve, at the spiral groove and along any plate applied to the shaft. For the elbow it is the ulnar nerve, which runs immediately adjacent to the medial column and is the nerve injured in elbow arthroplasty and its revision. Two points make the revision case different from a primary: the nerve has usually been handled or transposed at the index operation, so it may not lie where the anatomy says it should; and it is frequently encased in scar. Identify and protect it deliberately rather than assuming its position - the detail of its management in elbow arthroplasty, along with triceps insufficiency, is in Total Elbow Arthroplasty.
A total elbow arthroplasty carries a lifelong lifting restriction of roughly 2 to 5 kg. It is not a conservative suggestion for the early post-operative period - it is permanent, and it exists because load through a linked or semi-constrained elbow drives bushing wear, aseptic loosening and periprosthetic fracture. Non-compliance is a recognised route to early failure.
That has two consequences for this subject. First, it is prevention: the counselling given after the index arthroplasty is the main modifiable determinant of whether a periprosthetic fracture happens at all, so it is worth restating at every review rather than once at discharge. Second, it is a diagnostic clue: a periprosthetic fracture or a loose component in a patient who reports adhering to the limit should prompt a look for another explanation - infection, or a fall that was itself a warning about bone quality and balance - rather than being attributed to activity by default.
Don't Forget the Scapular Side
The humeral-stem classifications describe only one half of the shoulder. The scapular side has its own important periprosthetic fractures, especially after reverse total shoulder arthroplasty:
- Acromial and scapular-spine stress/insufficiency fractures - a recognised reverse-TSA complication caused by deltoid over-tensioning/lengthening (the deltoid is the prime mover after a reverse). They present as new pain and loss of elevation weeks to months after surgery and are graded by the Levy classification (type 1 anterior acromion / middle-deltoid origin, type 2 posterior acromion to the scapular spine, type 3 the base of the scapular spine). Most are managed non-operatively (immobilisation); ORIF is reserved for displaced scapular-spine fractures and even then has high nonunion/complication rates, and outcomes are often worse after such a fracture.
- Glenoid / baseplate periprosthetic fracture - intra-operative or from a fall, threatening baseplate fixation and sometimes needing revision.
- Differentiate an acromial fracture from a congenital os acromiale (an unfused apophysis - typically bilateral with smooth corticated margins).
The deltoid-tensioning mechanism and the reverse design are developed in Reverse Total Shoulder Arthroplasty and Rotator Cuff Arthropathy, and the unfused apophysis in Os Acromiale.
Remember the scapular side: after reverse TSA, deltoid over-tensioning causes acromial/scapular-spine stress fractures (new pain + loss of elevation; Levy types 1-3), usually treated non-operatively (ORIF only for displaced scapular-spine fractures, high nonunion), plus glenoid/baseplate periprosthetic fracture. Distinguish an acromial fracture from os acromiale.
Why They Matter & How to Classify
As shoulder and elbow arthroplasty become more common (especially reverse total shoulder arthroplasty and total elbow arthroplasty for fracture and arthritis in the elderly), periprosthetic fractures around these implants are an increasingly frequent and challenging complication. They usually occur in osteoporotic bone with limited bone stock, often intra-operatively or from a low-energy fall. The key to management - exactly as at the hip - is to characterise the fracture location, the implant stability, and the bone quality.
Mnemonics & Memory Aids
STEM
Hook:Around a STEM: classify by the tip, judge stability, and augment osteoporotic bone.
FIX-OR-REVISE
Hook:Fixed = fix; loose = revise (long stem) - the same upper-limb Vancouver logic.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“An elderly patient with a reverse total shoulder replacement falls and sustains a periprosthetic humeral fracture. How do you classify it, and what determines your treatment?”
“How is the approach to a periprosthetic fracture around a total elbow replacement classified and managed, and why is it challenging?”
General
- Rising with shoulder/elbow arthroplasty; usually osteoporotic elderly bone
- Vancouver-style logic: fracture location + implant stability + bone quality
- Identify implant + stem fixation; CT; exclude infection before revision
Shoulder (humerus)
- Classify relative to stem tip: Wright & Cofield A (at/proximal), B (around/just distal), C (distal)
- Wright & Cofield most reliable; overall agreement only moderate
- Strut allograft augments osteoporotic fixation (Worland B/C); protect radial nerve
Elbow (total elbow arthroplasty)
- Mayo (O'Driscoll-Morrey): I articulation/columns, II along stem (well-fixed vs loose), III beyond stem
- Thin ulna + condylar bone loss -> difficult fixation; strut graft/revision implants
- Type II subdivided by stem fixation
Treatment principle
- Well-fixed implant: ORIF (long plate, cerclage, strut allograft) or non-op (stable patterns)
- Loose implant: revise to long-stem component bypassing the fracture
- Augment osteoporotic bone; optimise the (usually elderly) patient
Evidence & Key Studies
Periprosthetic humerus fractures after shoulder arthroplasty: an evaluation of available classification systems
- Compared four periprosthetic-humerus-fracture classifications (Wright & Cofield, Campbell, Worland, Groh) for reliability across 34 fractures.
- The Wright & Cofield system had the greatest intraobserver and interobserver reliability; all systems showed only moderate interobserver agreement (and moderate agreement on preferred management).
- Highlights the need for a more reliable classification and a standardised treatment algorithm for periprosthetic humerus fractures.
Posterior approach with posterior locking plate and anterior strut allograft for periprosthetic humeral fractures after reverse total shoulder arthroplasty
- In 18 elderly patients with periprosthetic humeral fractures after reverse shoulder arthroplasty, a posterior approach with a posterior plate plus anterior strut allograft and cerclage achieved consolidation in all (mean 4.2 months) with good function.
- Treatment must consider fracture location, displacement and local bone quality; the technique is applicable to Worland B/C-type fractures.
- Strut allograft augmentation is useful for fixation in osteoporotic periprosthetic humeral bone.
The shoulder classification comparison (Wright & Cofield most reliable; only moderate agreement overall) comes from the cited Kuhn study, and the strut-allograft fixation approach from the cited Vicenti series. The Mayo (O'Driscoll & Morrey) total-elbow-arthroplasty classification and the Vancouver- style 'location + implant stability + bone quality' treatment principle are standard, well-established teaching applied from the hip. The lifelong 2-to-5 kg total elbow weight restriction is taken from Total Elbow Arthroplasty so the two pages carry the same figure. (See also THA Periprosthetic Fractures, TKA Periprosthetic Fractures for the Vancouver and Rorabeck systems this reasoning is borrowed from, and Periprosthetic Joint Infection for the work-up that must precede any revision.)