U-shaped Sacral Fracture / Lumbosacral Dissociation
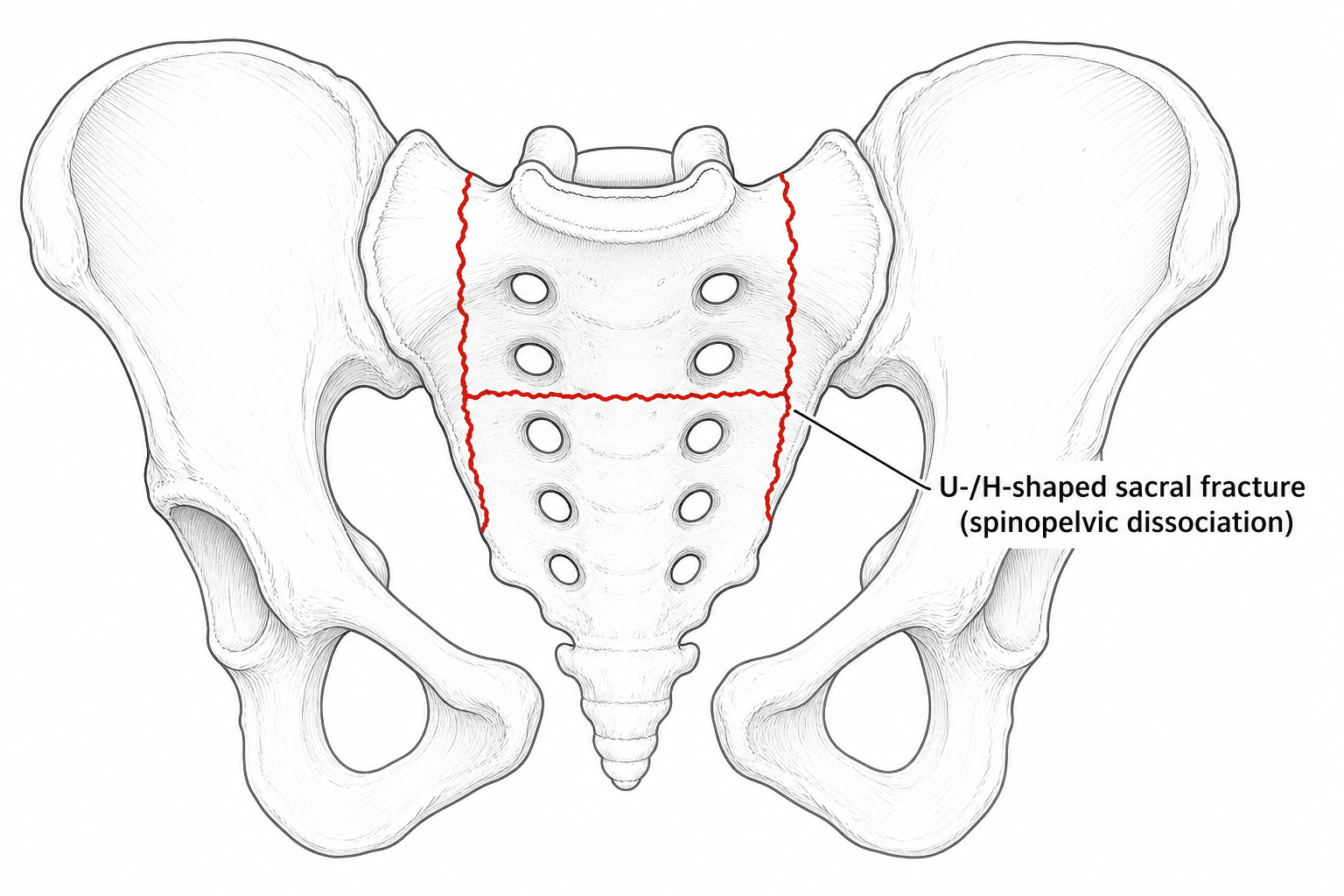
- Traumatic spinopelvic (lumbosacral) dissociation is a TRANSVERSE sacral fracture combined with BILATERAL vertical (longitudinal) sacral fractures, which together DISCONNECT the upper-central sacrum and the spine above it from the rest of the sacrum/pelvis - producing the 'U-shaped' (also H-, Y-, lambda- or T-shaped) sacral fracture.
- It is a RARE, HIGH-ENERGY axial-loading injury - classically a fall from height ('jumper's fracture') or high-speed collision - and is HIGHLY UNSTABLE, with a HIGH INCIDENCE of NEUROLOGICAL injury (cauda equina / sacral nerve roots: bladder, bowel, sexual and saddle dysfunction).
- It is EASILY MISSED and diagnosis is often DELAYED because patients usually have severe associated (poly)trauma and the TRANSVERSE component is hard to see on the AP pelvis - look for it on the LATERAL sacral view (sacral kyphosis/step) and confirm with CT; if missed it leads to progressive deformity and chronic pain.
- The TRANSVERSE component is graded by the ROY-CAMILLE classification (Type 1 flexion/kyphosis, Type 2 flexion + posterior translation, Type 3 extension + anterior translation, Type 4 comminuted), and the vertical components are usually DENIS ZONE 3 (central) - the zone with the highest neurological risk.
- Imaging requires plain pelvic radiographs (AP, INLET, OUTLET), a LATERAL SACRAL radiograph, and a CT with reconstructions to define the pattern; MRI assesses the lumbosacral roots/cauda equina.
- THE HONEST OUTCOME FIGURE: in 36 consecutive H-type dissociations treated with lumbopelvic fixation and decompression, excellent or good radiological reduction of the VERTICAL components was achieved in EVERY patient, and yet 15 (42%) still had a POOR CLINICAL OUTCOME. A satisfactory postoperative film is not a satisfactory patient, and a substantial minority recover incompletely - which is what consent should reflect.
- WHAT PREDICTS OUTCOME IS THE TRANSVERSE FRACTURE AND THE QUALITY OF REDUCTION: initial translational displacement predicted neurological recovery (p = 0.038) and clinical score (p < 0.001), with COMPLETELY displaced fractures faring worse than PARTIALLY displaced; and the displacement and kyphosis LEFT BEHIND after fixation also predicted the clinical score (p = 0.011 and p = 0.018). Reduction quality is the variable the surgeon controls that demonstrably changes the result.
- WHAT DID NOT PREDICT OUTCOME is examined as a trap: ROY-CAMILLE TYPE (2 versus 3) was not prognostic of neurological impairment, and neither were age, sex, ISS, the TIMING of surgery, or whether a SACRAL LAMINECTOMY was performed. Roy-Camille remains the way to describe the transverse pattern, but the authors propose the more useful split of PARTIALLY versus COMPLETELY displaced. Do not over-read the negative findings - a series of 36 cannot exclude a timing effect, and an established cauda equina deficit is still decompressed.
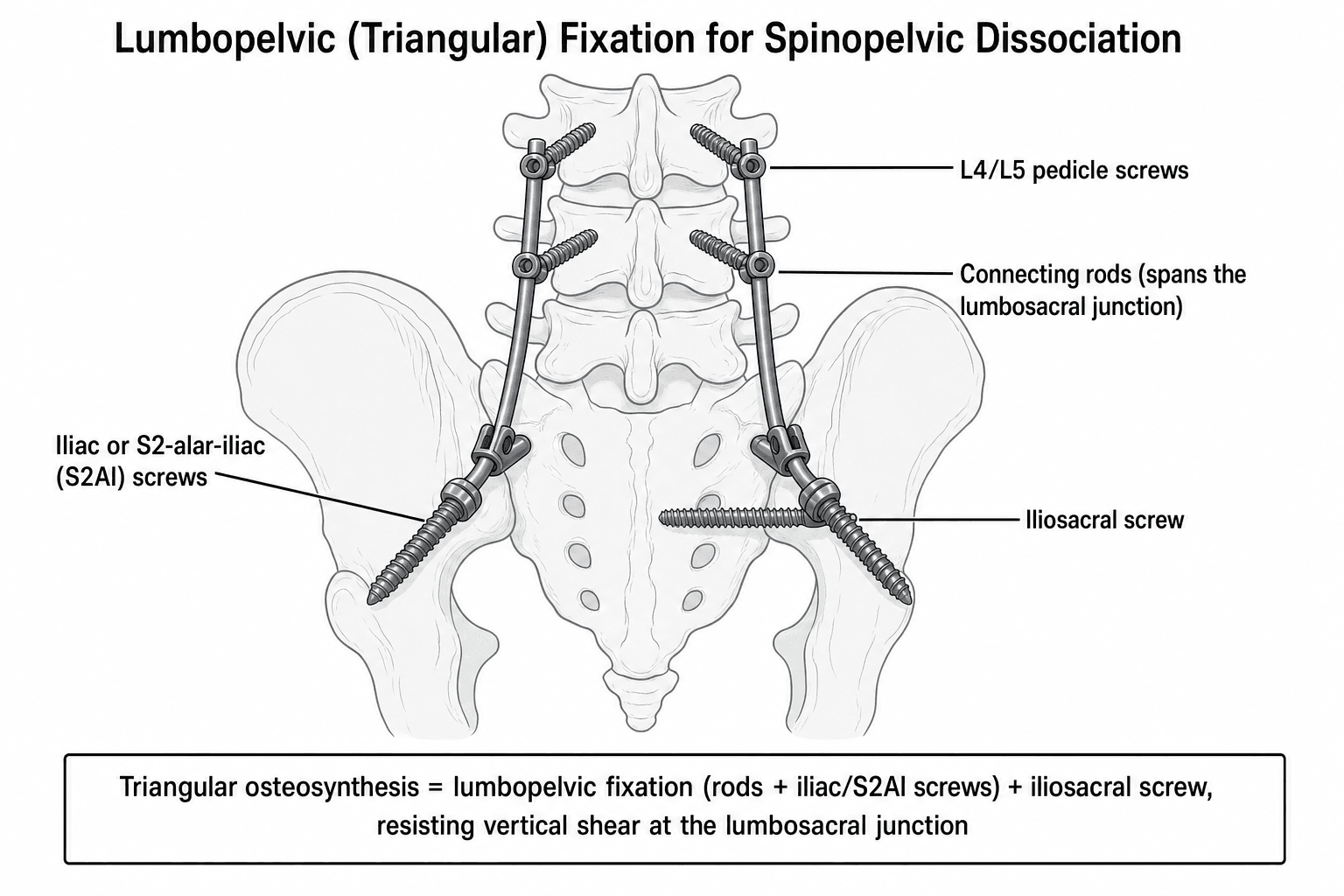
- Because the lumbopelvic junction is unstable, treatment is usually OPERATIVE: REALIGNMENT and LUMBOPELVIC FIXATION (spinopelvic fixation - e.g. L4/L5 pedicle to iliac or S2-alar-iliac screws, with or without iliosacral screws = TRIANGULAR OSTEOSYNTHESIS) to restore stability and allow EARLY MOBILISATION, with SACRAL DECOMPRESSION of compromised nerve roots when there is neurological deficit or canal compromise.
- “Spinopelvic dissociation = transverse + bilateral vertical sacral fractures (U/H shape) separating spine from pelvis - high-energy, highly unstable, high neuro-injury rate.
- “It's easily missed: look for the transverse component on the LATERAL sacral view (sacral kyphosis) and CT; suspect it in a jumper/polytrauma patient with sacral neurology.
- “Treat with lumbopelvic (triangular) fixation +/- sacral decompression; classify the transverse part by Roy-Camille (zone 3 Denis = highest neuro risk).
- “Honest outcome: 42% of 36 had a POOR clinical outcome despite good radiological reduction of the vertical components in ALL of them. Consent for that.
- “Predicts outcome: transverse-fracture displacement (initial AND residual) and residual kyphosis. Does NOT predict: Roy-Camille type, age, ISS, timing of surgery, laminectomy.
- “Report the deficit as a Gibbons grade: 1 none, 2 sensory, 3 motor, 4 sphincter (bowel/bladder). Sphincter involvement recovers least reliably.
The patient is usually a polytrauma victim, and the transverse sacral component is hard to see on the AP pelvis. Look at the LATERAL sacrum (kyphosis/step), get a CT, and actively suspect it after a fall from height or with unexplained sacral neurology.
The vertical fractures are usually Denis zone 3 (central canal/transforaminal), so cauda equina and sacral-root injury is common - assess bladder, bowel, perianal sensation and sexual function in every suspected case.
What It Is & Why It Happens
In spinopelvic dissociation, bilateral vertical sacral fractures (one through each ala/foraminal region) are joined by a transverse fracture of the sacral body, so the upper-central sacrum - and the entire spine above it - is mechanically dissociated from the rest of the sacrum and the pelvis. The configuration of the transverse and vertical lines gives the characteristic shapes - 'U', 'H', 'Y', 'lambda' or 'T'. The mechanism is high-energy axial loading, classically a fall from a height (the 'jumper's fracture', often with calcaneal/tibial-plateau/spinal burst fractures) or a high-speed collision, so it is typically part of severe polytrauma.
Classification
- Pattern
- Simple flexion - kyphotic ANGULATION of the upper sacral fragment (no translation)
- Pattern
- Flexion with POSTERIOR translation of the upper fragment
- Pattern
- Extension with ANTERIOR translation of the upper fragment
- Pattern
- Comminuted/segmental fracture of the S1 body
The vertical components of the sacral fracture are graded by the Denis zones - Zone 1 (lateral to the foramina/ala), Zone 2 (transforaminal) and Zone 3 (medial to the foramina / central canal). Spinopelvic dissociation involves the central sacrum (Zone 3) and the transverse canal, which is why the neurological-injury rate is high (cauda equina and sacral roots controlling bladder, bowel and sexual function). The Roy-Camille type communicates the direction of the transverse displacement, but note that comparing type 2 against type 3 has not been shown to predict neurological impairment - what predicts outcome is the degree of displacement of the transverse fracture (partially versus completely displaced), and how much displacement and kyphosis are left behind after fixation.
Assessment
- Pelvic radiographs: AP, inlet and outlet views
- LATERAL sacral radiograph - key to seeing the transverse component / sacral kyphosis
- CT with reconstructions - essential to define the full pattern (the diagnosis is often made here)
- MRI to evaluate the lumbosacral roots / cauda equina
- High-energy mechanism (fall from height, MVC) - treat as polytrauma (ATLS)
- Examine sacral neurology: bladder/bowel function, perianal sensation, anal tone, sexual function, lower-limb roots
- Inspect the soft tissues (degloving/Morel-Lavallée); assess associated spinal/limb injuries
Management
Because the lumbopelvic junction is grossly unstable, treatment is usually surgical, with three aims:
- Realignment / reduction of the displaced/kyphotic sacrum.
- Stable fixation of the lumbopelvic junction - LUMBOPELVIC (spinopelvic) FIXATION, connecting the lower lumbar spine (L4/L5 pedicle screws) to the pelvis (iliac or S2-alar-iliac (S2AI) screws), often combined with iliosacral screws as 'triangular osteosynthesis'. This provides robust, load-sharing fixation that resists the high shear at the lumbosacral junction and allows EARLY MOBILISATION of the polytrauma patient.
- Sacral decompression (e.g. sacral laminectomy / foraminal decompression) when there is a neurological deficit or canal/root compromise. A small series of 14 patients using lumbopelvic fixation with S2AI screws reported good reduction and function, union in all and neurological recovery, with low complication rates - but that optimism should be set against a larger series of 36 in which 42% had a poor clinical outcome despite good radiological reduction of the vertical components in every patient. Counsel accordingly. (Minimally displaced, neurologically intact fractures may occasionally be managed non-operatively, but the unstable, displaced or neurologically involved patterns need fixation.)
The Sacral Kyphosis: Why You Must Reduce It
Realigning the kyphotic sacrum matters, and the lateral view showing a sacral kyphosis/step explains why. The transverse fracture lets the upper sacrum and the spine above it flex (and often translate), producing a lumbosacral kyphosis. That angulation and translation narrows the sacral canal and tents/compresses the cauda equina and sacral roots, so it directly contributes to the neurological deficit; it also unbalances sitting and the spinopelvic sagittal alignment and, if left, causes progressive deformity and chronic pain.
So reduction is therapeutic, not cosmetic: correcting the kyphosis indirectly decompresses the canal and restores sitting/sagittal balance. The principle is to realign the kyphosis - typically prone positioning (which itself helps extend the lumbosacral junction), restoring sacral lordosis and correcting the angulation/translation, frequently using the lumbopelvic instrumentation as the reduction tool (cantilever / compression-distraction across the construct), under intra-operative neuromonitoring because reducing the deformity moves the already-compromised roots. Indirect reduction may relieve canal compromise, but a true deficit or persistent canal/root compression still warrants direct decompression.
This is the part of the operation with the best evidence behind it: in the 36-patient series, residual translational displacement and residual kyphosis of the transverse fracture both predicted the clinical outcome, while Roy-Camille type, timing and laminectomy did not. Reduction quality is the variable the surgeon controls that demonstrably changes the result. (The spinopelvic sagittal parameters are developed in Spinopelvic Parameters and the construct detail in Sacropelvic Fixation.)
The sacral kyphosis is not cosmetic - it narrows the canal and compresses the cauda equina and unbalances sitting. Reduce it (prone positioning, restore sacral lordosis, reduce via the construct under neuromonitoring) and it indirectly decompresses - but a true deficit/canal compression still needs direct decompression.
Sacral Roots: The Deficit and Its Recovery
A sacral neurological examination and counselling about incomplete recovery both rest on the same anatomy. The sacral canal carries the cauda equina and the sacral nerve roots: S2-S4 provide the parasympathetic control of bladder and bowel, the anal and urethral sphincters, perianal (saddle) sensation and sexual function, while S1 contributes to plantarflexion. A central, canal-involving (Denis zone 3) fracture therefore characteristically produces a cauda-equina picture - urinary retention/overflow, bowel and sexual dysfunction, saddle anaesthesia and reduced anal tone and voluntary squeeze - and because the fracture is central the deficit is often bilateral. That is why the examination must include bladder and bowel function (with a post-void residual), perianal sensation, anal tone and sexual function, and a PR examination.
For prognosis: many patients recover at least partially after realignment (indirect decompression) and direct decompression of compromised roots, but recovery is unpredictable, and bladder, bowel and sexual function recover the least reliably - so counsel honestly, and note that in the largest series available 42% had a poor clinical outcome. Neurological status is tracked with the Gibbons grade (1 no deficit, 2 sensory, 3 motor, 4 sphincter), and decompression is undertaken for an established deficit or canal compromise, with wider sacral-fracture practice favouring within about 24 to 72 hours - while recognising that in the 36-patient series neither the timing of surgery nor whether a laminectomy was performed reached statistical significance, and the quality of reduction did. (General cauda equina syndrome is developed in Cauda Equina Syndrome and the root anatomy in Lumbosacral Plexus Anatomy; what follows here is the sacral-root deficit specific to this fracture.)
A central (Denis zone 3) sacral fracture threatens S2-S4 → a cauda-equina picture (retention, bowel/sexual dysfunction, saddle anaesthesia, reduced anal tone), often bilateral. Examine bladder/bowel/perianal/ sexual in every case; after realignment and decompression recovery is partial and least reliable for bladder, bowel and sexual function.
What Actually Predicts Outcome - and What Does Not
The Uncomfortable Headline
In 36 consecutive H-type spinopelvic dissociations treated with lumbopelvic fixation and neural decompression over an 18-year period, with a minimum 18-month follow-up: excellent or good radiological results were achieved in the vertical components in every single patient, and yet 15 of the 36 (42%) still had a poor clinical outcome.
That single sentence reframes the operation. Getting the vertical fractures to look right on the postoperative film is not the same as getting the patient right, and a substantial minority do badly despite a technically satisfactory construct. It is the honest figure to carry into a consent discussion.
It Is the Transverse Fracture, and the Reduction, That Matter
- Association with outcome
- PREDICTS neurological recovery and clinical outcome - completely displaced fractures did worse than partially displaced ones
- Significance
- p = 0.038 for neurological recovery; p < 0.001 for clinical score
- Association with outcome
- PREDICTS clinical outcome - what you leave behind counts
- Significance
- p = 0.011
- Association with outcome
- PREDICTS clinical outcome
- Significance
- p = 0.018
- Association with outcome
- NOT associated with outcome, and not prognostic of neurological impairment
- Significance
- Not significant
- Association with outcome
- NOT associated with outcome in this series
- Significance
- Not significant
- Association with outcome
- NOT associated with outcome
- Significance
- Not significant
- Association with outcome
- NOT associated with outcome
- Significance
- Not significant
Two consequences follow, and both are examinable because they run against the intuitive answer.
Roy-Camille classifies the injury; it does not predict it. The type describes the direction of the transverse displacement and remains the standard way to communicate the pattern, but comparing type 2 against type 3 did not predict neurological impairment. The authors instead propose the simpler and more useful split of the transverse fracture into partially displaced versus completely displaced, which did predict the rate of neurological recovery.
Accurate reduction is the variable the surgeon controls that actually matters. Initial displacement is fixed by the injury, but residual displacement and residual kyphosis are chosen in theatre - and both predicted the clinical score. This is the evidence behind reducing the sacral kyphosis rather than merely spanning it.
That timing of surgery and laminectomy were not statistically associated with outcome in a series of 36 is not evidence that decompression can be delayed or omitted. An established cauda equina deficit with canal compromise is still decompressed, and wider sacral-fracture practice favours doing so within about 24 to 72 hours. A single retrospective series of this size is underpowered to exclude a timing effect - what it does show positively is that the quality of reduction carried the outcome.
Grading the Deficit: the Gibbons Score
Neurological status in these injuries is reported with the Gibbons grade, which measures the deficit itself rather than the fracture's location: Grade 1 no deficit; Grade 2 sensory deficit only; Grade 3 lower-limb motor deficit; Grade 4 bowel or bladder (sphincter) dysfunction. The change in Gibbons grade is the standard way outcome is reported after decompression and fixation, and higher grades - sphincter involvement above all - recover least reliably. Record it alongside a documented perianal (S2-S4) examination and bulbocavernosus reflex so the baseline is unambiguous.
Quote the honest number: 42% of 36 had a poor clinical outcome despite good radiological reduction of the vertical components in all of them. What predicted outcome was displacement of the TRANSVERSE fracture - initial, and crucially residual - plus residual kyphosis. What did not: Roy-Camille type, age, ISS, timing of surgery and laminectomy. Report the deficit as a Gibbons grade (1 none, 2 sensory, 3 motor, 4 sphincter).
Mnemonics & Memory Aids
U-SHAPE
Hook:U-SHAPE: the spine separates from the pelvis - high-energy, high-neuro, see it on the lateral/CT, fix it lumbopelvic.
ROY
Hook:Roy-Camille: 1 angulation, 2 posterior, 3 anterior translation, 4 comminuted.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient who fell from a height has sacral pain and difficulty voiding. What injury must you consider, what is the fracture pattern, and how would you image and assess it?”
“CT confirms a U-shaped sacral fracture with kyphotic displacement and a cauda equina deficit. How would you classify and manage it?”
What it is
- Transverse + bilateral vertical sacral fractures = U/H/Y/lambda shape
- Spine dissociated from pelvis - highly unstable
- High-energy (fall from height/jumper's fracture); usually polytrauma
Classify
- Transverse component: Roy-Camille 1 (flexion/kyphosis), 2 (flexion+posterior), 3 (extension+anterior), 4 (comminuted)
- Vertical components: Denis zone 3 (central) - highest neuro risk
- High rate of cauda equina/sacral-root injury
Diagnose
- Easily missed - AP/inlet/outlet + LATERAL sacrum (kyphosis) + CT (+/- MRI)
- Full sacral neuro exam (bladder/bowel/perianal/sexual)
- Screen for associated spinal/limb injuries
Treat
- Realign + lumbopelvic (spinopelvic) fixation - L4/L5 to iliac/S2AI screws +/- iliosacral (triangular osteosynthesis)
- Sacral decompression for neurological deficit/canal compromise (wider practice: within ~24-72 h)
- Robust fixation -> early mobilisation; counsel re incomplete neuro recovery
Outcome & predictors
- 42% of 36 had a POOR clinical outcome despite good radiological reduction in ALL
- PREDICTS: transverse-fracture displacement, initial and residual; residual kyphosis
- Completely displaced does worse than partially displaced transverse fracture
- DOES NOT PREDICT: Roy-Camille type, age, sex, ISS, timing of surgery, laminectomy
- Gibbons grade: 1 none / 2 sensory / 3 motor / 4 sphincter - sphincter recovers worst
- Accurate reduction is the surgeon-controlled variable that changes the result
Evidence & Key Studies
Traumatic spinopelvic dissociation or U-shaped sacral fracture: a review of the literature
- Spinopelvic dissociation is a rare high-energy injury - a transverse sacral fracture with bilateral sacral fracture-dislocations - with a high incidence of neurological complications.
- It is easily missed/delayed because patients commonly have severe associated injuries; if untreated it leads to progressive deformity and chronic pain. Imaging needs AP/inlet/outlet pelvis, a lateral sacral radiograph and CT.
- Early realignment and fixation of the unstable lumbopelvic junction (lumbopelvic fixation / triangular osteosynthesis) with decompression of compromised roots provides the best environment for early mobilisation.
Lumbopelvic fixation with S2 alar-iliac screws for U-shaped sacral fractures
- In 14 patients with U-shaped sacral fractures treated by lumbopelvic fixation with S2 alar-iliac (S2AI) screws, 92% had excellent/good reduction and 100% excellent/good pelvic function, with all fractures healed and neurological recovery in all.
- Complications were minimal (one superficial infection); no implant failure, loss of reduction or deep infection occurred.
- S2AI-screw lumbopelvic fixation gives firm fixation with low complication rates and supports early rehabilitation.
Factors associated with outcome of spinopelvic dissociation treated with lumbopelvic fixation
- Thirty-six consecutive H-type spinopelvic dissociations treated by lumbopelvic fixation and neural decompression over 18 years, minimum 18-month follow-up: excellent or good radiological results in the vertical components were achieved in ALL patients, yet 15 (42%) had a poor clinical outcome on the Pelvis Outcome Scale.
- Initial translational displacement of the TRANSVERSE fracture predicted neurological recovery by Gibbons score (p = 0.038) and final clinical score (p < 0.001), with completely displaced fractures faring worse than partially displaced ones; residual translational displacement (p = 0.011) and residual kyphosis (p = 0.018) also predicted clinical outcome.
- Roy-Camille classification (type 2 versus 3), age, sex, Injury Severity Score, timing of surgery and sacral laminectomy showed NO statistically significant association with outcome - the authors conclude Roy-Camille is not prognostic of neurological impairment and propose categorising the transverse fracture as partially versus completely displaced instead.
The injury definition, the missed-diagnosis pitfall, the imaging requirements and the lumbopelvic-fixation/triangular-osteosynthesis principle come from the cited Yi and Hak review. The S2AI lumbopelvic-fixation outcomes are the cited Luo series, which is 14 patients - small enough that its near-perfect results are quoted here alongside, not instead of, the larger figure. That larger figure, the predictors of outcome and all the negative findings - 42% poor outcome in 36 patients, the significance of initial and residual transverse displacement and residual kyphosis, and the absence of any significant association with Roy-Camille type, age, sex, ISS, timing of surgery or laminectomy - come from the cited Lindahl series, a single-centre retrospective cohort collected over 18 years.
Those negative findings are reported as measured rather than as recommendations: a series of 36 is underpowered to exclude a real effect of surgical timing, which is why an established deficit is still decompressed here, with the 24-to-72-hour window taken in substance from Sacral Fractures, where it is set out for sacral fractures generally with its own sources. The Gibbons grade definitions are likewise taken in substance from that page. The Roy-Camille classification of the transverse component and the Denis zones are standard, well-established teaching. (See also Pelvic Ring Injuries.)