Os Peroneum & Os Vesalianum
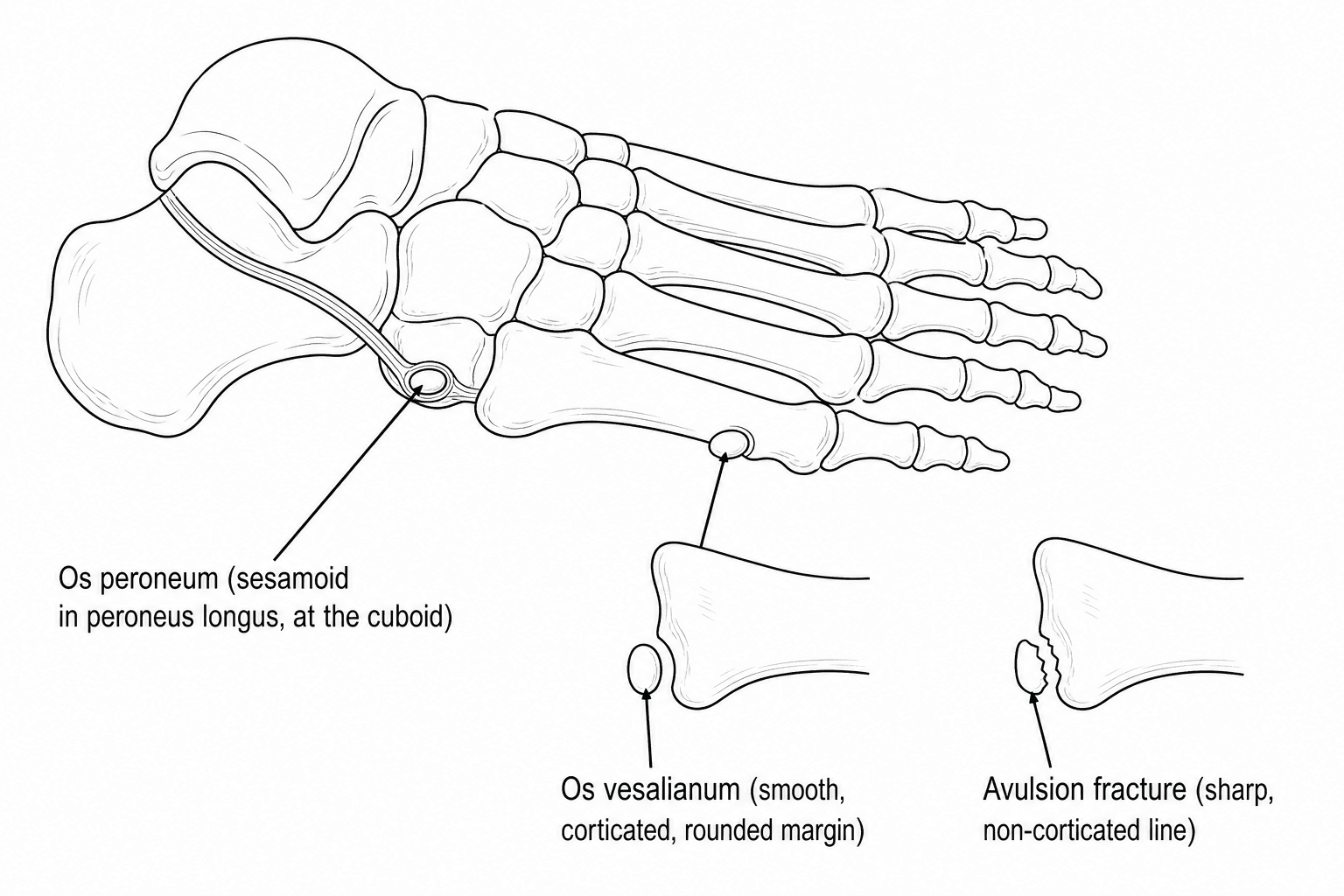
- The OS PERONEUM is a sesamoid bone within the peroneus longus tendon where the tendon turns around the cuboid; it is often an incidental, asymptomatic finding (sometimes bipartite/multipartite), but it can be the seat of the PAINFUL OS PERONEUM SYNDROME (POPS), a spectrum of disorders causing lateral and plantar-lateral foot pain.
- POPS has an ACUTE form - typically after a supination/inversion injury that fractures the os peroneum or ruptures the peroneus longus tendon - and a CHRONIC form from recurrent injury or healing with calcific remodelling, producing peroneus longus tenosynovitis/tendinopathy and a risk of subsequent tendon rupture; simple acute cases can settle with a short course of a non-steroidal anti-inflammatory and rest.
- A KEY EXAM POINT: on radiographs, marked DISPLACEMENT or DIASTASIS of the os peroneum (or wide separation of a fractured/partitioned os, including proximal retraction above the level of the ankle) is used as an imaging SURROGATE for a complete PERONEUS LONGUS TEAR; MRI is needed to characterise the tendon, and the assumption of a complete tear from a retracted os is not absolute - some have only a partial tear.
- The OS VESALIANUM is a rare accessory ossicle at the BASE of the FIFTH METATARSAL, lying within or adjacent to the peroneus brevis insertion; the crucial distinction is from a fifth-metatarsal base AVULSION FRACTURE - the ossicle has smooth, corticated, rounded margins, sits proximal to the metatarsal base, is often bilateral, and the fracture line of an avulsion is sharp and non-corticated (comparison views of the other foot help).
- Other named accessory ossicles of the foot have their own considerations: the OS TRIGONUM (posterior talus, posterior ankle impingement) and the ACCESSORY NAVICULAR (medial navicular, posterior tibial tendon dysfunction) are covered on their own pages - the unifying principle is that an accessory ossicle is usually incidental and only relevant when it is SYMPTOMATIC and corresponds to the site of pain.
- MANAGEMENT of a painful accessory ossicle is NON-OPERATIVE first - activity modification, a period of immobilisation/orthoses, non-steroidal anti-inflammatories and physiotherapy - with SURGERY (excision of the ossicle, debridement or repair/reconstruction of the involved tendon, e.g. peroneus longus to brevis tenodesis where the longus is irreparable) reserved for refractory symptoms or an established tendon rupture; the decision is driven by symptoms and the tendon, not the incidental radiographic finding.
- “Os peroneum = sesamoid IN the peroneus longus at the cuboid; painful os peroneum syndrome (POPS) = lateral/plantar-lateral foot pain (acute # / PL rupture vs chronic tenosynovitis).
- “DISPLACED/DIASTATIC os peroneum (esp. proximally retracted) = surrogate for a PERONEUS LONGUS TEAR - get MRI to characterise the tendon.
- “Os vesalianum (5th-MT base, peroneus brevis) - distinguish from an AVULSION FRACTURE: smooth corticated rounded margins, often bilateral on comparison views, vs a sharp non-corticated fracture line.
Marked displacement/diastasis (especially proximal retraction) of the os peroneum is a surrogate for a peroneus longus rupture - get MRI to characterise the tendon. Do not dismiss it as 'just an ossicle'.
At the fifth-metatarsal base, a smooth, corticated, rounded ossicle (often bilateral) is an os vesalianum, not an avulsion fracture (sharp, non-corticated line). Comparison views help.
The Map: Which Ossicle, Where, and In Which Tendon
Accessory ossicles are common and mostly silent, so the useful knowledge is not a list of names but a map - where each one sits, which tendon it lies in, and what it is mistaken for. Almost every one of them becomes an exam question in the same two ways: is it an ossicle or a fracture, and is it the source of the pain.
- Where it sits / which tendon
- Plantar-lateral, in the PERONEUS LONGUS as it turns round the cuboid
- What it is mistaken for, and where it is covered
- Fracture of the ossicle - and a displaced one signals a peroneus longus tear (below)
- Where it sits / which tendon
- Proximal to the fifth-metatarsal base, at the PERONEUS BREVIS insertion
- What it is mistaken for, and where it is covered
- A zone 1 avulsion fracture (compared in detail below)
- Where it sits / which tendon
- Posterior talus - the unfused lateral tubercle of the posterior process, adjacent to the FHL groove
- What it is mistaken for, and where it is covered
- The cause of posterior ankle impingement, and easily confused with an elongated but FUSED Stieda process
- Where it sits / which tendon
- Medial navicular tuberosity, within or adjacent to the TIBIALIS POSTERIOR insertion
- What it is mistaken for, and where it is covered
- A navicular fracture; the symptomatic Geist type II has a shear-loaded synchondrosis
- Where it sits / which tendon
- Within the FHB tendons under the first metatarsal head; the TIBIAL (medial) sesamoid is the one usually bipartite
- What it is mistaken for, and where it is covered
- A sesamoid fracture - bipartite margins are smooth and corticated, and it is often bilateral
- Where it sits / which tendon
- Below the tip of the lateral or medial malleolus
- What it is mistaken for, and where it is covered
- An old avulsion of the ligament attachment, and in a child an unfused ossification centre
- Where it sits / which tendon
- Dorsal midfoot and dorsal talar neck
- What it is mistaken for, and where it is covered
- Dorsal osteophytes or chip fractures; occasionally symptomatic against footwear or, for the os intermetatarseum, implicated in deep peroneal nerve compression
Each of the entries above that carries its own clinical syndrome is developed separately: Os Trigonum and Posterior Ankle Impingement, Accessory Navicular, Sesamoid Disorders for the bipartite hallux sesamoid, and Pseudo-Jones Fractures for the zone 1 avulsion that the os vesalianum imitates.
Two rules apply to all of them. An ossicle is corticated on every surface, because it has always been a separate bone, while a fracture fragment has at least one raw, non-corticated edge that matches a defect in the parent bone. And an ossicle only matters if the tenderness sits precisely on it - incidental ossicles are common enough that finding one on a radiograph explains nothing by itself.
Os Peroneum & Painful Os Peroneum Syndrome (POPS)
The os peroneum is a sesamoid bone within the peroneus longus tendon where the tendon turns around the cuboid to cross the sole. It is frequently an incidental, asymptomatic finding (and may be bipartite or multipartite). The painful os peroneum syndrome (POPS) is a spectrum of disorders producing lateral and plantar-lateral foot pain centred on the cuboid. The acute form follows trauma - classically a supination/inversion injury that fractures the os peroneum or ruptures the peroneus longus tendon; the chronic form arises from recurrent injury or healing with calcific remodelling, with peroneus longus tenosynovitis/tendinopathy and a risk of later tendon rupture. Simple acute presentations may settle with a short course of a non-steroidal anti-inflammatory and rest.
On radiographs, marked displacement or diastasis of the os peroneum (or wide separation of a fractured/partitioned os, including proximal retraction of a fragment above the level of the ankle) is used as an imaging surrogate for a complete peroneus longus tendon tear. MRI characterises the tendon and surrounding soft tissue. The relationship is not absolute - a retracted proximal moiety can occur with only a partial peroneus longus tear (the os occupies part of the tendon's cross-section and the eccentric intact fibres remain in continuity) - so MRI provides the full description rather than the radiograph alone.
Os Vesalianum vs Fifth-Metatarsal Base Avulsion
- Os vesalianum (accessory ossicle)
- Smooth, corticated, rounded
- Avulsion fracture (zone 1)
- Sharp, non-corticated fracture line
- Os vesalianum (accessory ossicle)
- Proximal to the 5th-MT base (in peroneus brevis)
- Avulsion fracture (zone 1)
- At the 5th-MT tuberosity/base
- Os vesalianum (accessory ossicle)
- Often bilateral (comparison views help)
- Avulsion fracture (zone 1)
- Unilateral, follows the injury
- Os vesalianum (accessory ossicle)
- Developmental (incidental); pain if symptomatic
- Avulsion fracture (zone 1)
- Inversion injury - acute pain/tenderness
- Os vesalianum (accessory ossicle)
- No acute injury / chronic/incidental
- Avulsion fracture (zone 1)
- Acute injury with focal bony tenderness
A rounded, corticated ossicle at the fifth-metatarsal base - especially if bilateral and without an acute injury - is an os vesalianum, not an avulsion fracture. Conversely, do not dismiss a genuine zone 1 avulsion as an ossicle. The os vesalianum is usually asymptomatic and incidental; treat it only when it is the clear source of symptoms, and then non-operatively first.
The Sobel Classification of the Os Peroneum
Displacement or diastasis acts as a surrogate for a peroneus longus tear, and the framework that grades it is the Sobel classification of the painful os peroneum syndrome, which maps the os-peroneum appearance onto the peroneus longus pathology:
- An acute os-peroneum fracture, or diastasis of a multipartite os - both implying a partial peroneus longus tear at the os.
- A chronic/healed fracture or diastasis with callus / calcific remodelling - implying peroneus longus tenosynovitis/stenosis.
- Attrition or partial tear of the peroneus longus without a fracture, with the os entrapped at the peroneal tubercle / cuboid tunnel.
- Frank rupture of the peroneus longus, with proximal retraction of the os peroneum.
- A large/hypertrophied peroneal tubercle causing attrition.
So the degree of os displacement/diastasis/retraction maps onto the severity of the peroneus longus injury - which is why a retracted os signals a complete tear - but (per the evidence above) MRI is still required, because a retracted os can occur with only a partial tear. (Repair, tenodesis and the rest of the surgical management of the torn tendon are in Peroneal Tendon Tears.)
The Sobel classification grades the os peroneum onto the peroneus longus injury: fracture/diastasis = partial tear; healed with callus = tenosynovitis/stenosis; attrition without fracture = entrapment; proximal retraction of the os = frank rupture; plus a hypertrophic peroneal tubercle. Retraction signals a complete tear - but confirm with MRI (it can be only partial).
Management Principles
- Non-operative first: activity modification, a period of immobilisation and/or orthoses, non-steroidal anti-inflammatories and physiotherapy - most symptomatic ossicles settle.
- Image to define the tendon: for POPS, a displaced/diastatic os peroneum should prompt MRI to define the peroneus longus (intact, partial tear, complete rupture).
- Surgery for refractory pain or tendon rupture: excision of the symptomatic ossicle, with debridement or repair/reconstruction of the involved tendon - where the peroneus longus is irreparable, a peroneus longus to brevis tenodesis restores eversion.
- Decide on symptoms and the tendon - an incidental, smooth, corticated ossicle that does not match the site of pain needs no treatment.
The clinically important lesson of the painful os peroneum syndrome is that a displaced or diastatic os peroneum on a radiograph is not simply an incidental ossicle - it can be the only clue to a peroneus longus tendon tear, which alters management (immobilisation/repair rather than reassurance) and, if missed, leaves a weak eversion and ongoing lateral-foot pain. Whenever the os peroneum is displaced, fragmented, or proximally retracted, obtain an MRI to characterise the tendon before deciding treatment. Equally, at the fifth-metatarsal base, do not mislabel an acute zone 1 avulsion fracture as an os vesalianum (or vice versa); use the margin characteristics and comparison views, and correlate with the history and the site of tenderness.
Examining the Painful Lateral Foot
- Examination: localise tenderness over the os peroneum at the plantar-lateral cuboid; reproduce pain and look for weakness on resisted eversion and on resisted first-ray plantarflexion (the peroneus longus plantarflexes the first ray); inspect for a cavovarus foot (predisposes to lateral/peroneal overload) and check that the peroneal tendons do not sublux behind the fibula on resisted dorsiflexion-eversion.
- The differential of lateral foot pain (do not anchor on the ossicle): peroneal tendon tear or subluxation, cuboid syndrome, calcaneocuboid osteoarthritis, a lateral process of talus fracture, a fifth-metatarsal-base avulsion / Jones / stress fracture, and lateral ankle pathology.
- The diagnostic logic: a symptomatic ossicle reproduces pain at its own site; an incidental one does not. Image with weight-bearing radiographs (plus comparison views), MRI for the tendon, and occasionally CT or a bone scan to confirm that the ossicle is the symptomatic source.
Each of those alternatives is developed in its own right: Peroneal Tendon Disorders, Peroneal Tendon Subluxation, Cuboid Fractures, Calcaneocuboid Arthritis, Lateral Process of Talus Fractures, Jones Fractures and Fifth Metatarsal Stress Fractures.
Examine for POPS: tenderness at the plantar-lateral cuboid, pain/weakness on resisted eversion and first-ray plantarflexion, a cavovarus foot and peroneal subluxation. The lateral-foot differential - peroneal tear/subluxation, cuboid syndrome, calcaneocuboid OA, lateral-process-of-talus and fifth-metatarsal fractures - means you treat the ossicle only when it reproduces pain at its site.
Mnemonics & Memory Aids
POPS
Hook:POPS: Peroneus longus sesamoid, Os displaced = tear (MRI), Pain lateral foot, Start non-operative.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has chronic lateral midfoot pain. The radiograph shows a displaced, fragmented os peroneum. What is your concern and what do you do?”
“A radiograph of an ankle injury shows a bony fragment at the base of the fifth metatarsal. How do you decide whether it is an avulsion fracture or an os vesalianum?”
Os peroneum
- Sesamoid within the peroneus longus at the cuboid (often incidental/bipartite)
- Painful os peroneum syndrome (POPS): acute (# / PL rupture) vs chronic (tenosynovitis)
- Displaced/diastatic/retracted os = surrogate for a peroneus longus tear - get MRI
Os vesalianum
- Accessory ossicle at the 5th-MT base (peroneus brevis insertion)
- Smooth/corticated/rounded, often bilateral - NOT an avulsion fracture
- Avulsion = sharp non-corticated line, unilateral, post-inversion (comparison views help)
Management
- Non-operative first: activity modification, immobilisation/orthoses, NSAIDs, physiotherapy
- Surgery for refractory pain or tendon rupture: ossicle excision + tendon repair/reconstruction
- Irreparable peroneus longus -> peroneus longus to brevis tenodesis
Don't forget
- Os trigonum (posterior talus) and accessory navicular have their own pages
- Treat the symptom and the tendon, not the incidental ossicle
- Correlate radiograph with history + site of tenderness
Evidence & Key Studies
Painful os peroneum syndrome: presentation and management
- The painful os peroneum syndrome is subdivided into acute and chronic forms; the acute presentation usually follows trauma - most commonly a supination or inversion of the ankle - which can fracture the os peroneum or rupture the peroneus longus tendon.
- The chronic presentation results from recurrent foot injury or healing of a fracture with calcific remodelling of the sesamoid, producing peroneus longus tendinopathy/tenosynovitis and a risk of subsequent tendon rupture.
- MRI characterised the os peroneum, surrounding soft-tissue swelling and peroneus longus tendinopathy; the reported case settled with a short course of a non-steroidal anti-inflammatory.
Retracted os peroneum with partial integrity of the peroneus longus tendon
- Marked displacement of the proximal fragment of the os peroneum on radiographs is often used as an imaging surrogate for a complete peroneus longus tendon tear.
- A retracted proximal os peroneum (even above the level of the ankle) can occur with only an incomplete peroneus longus tear, because the os occupies part of the tendon's cross-section and eccentric intact fibres remain in continuity.
- MRI is required to provide a full description of the tendon, and a complete tear should not be assumed from a retracted os on radiography alone.
The acute/chronic spectrum of the painful os peroneum syndrome and its conservative resolution come from the cited Henrique Segatt report, and the use (and limitation) of a displaced/retracted os peroneum as a surrogate for a peroneus longus tear - with MRI for full characterisation - from the cited Lee report. The anatomy of the os peroneum (sesamoid in the peroneus longus at the cuboid) and os vesalianum (fifth metatarsal base, peroneus brevis) and their distinction from avulsion fractures are standard, well-established teaching, as is the map of the named ossicles and the tendons they lie within. (See also Os Trigonum, Accessory Navicular, Sesamoid Disorders, Peroneal Tendon Disorders and Pseudo-Jones Fractures.)