Flexor-Tendon Imbalance Phenomena
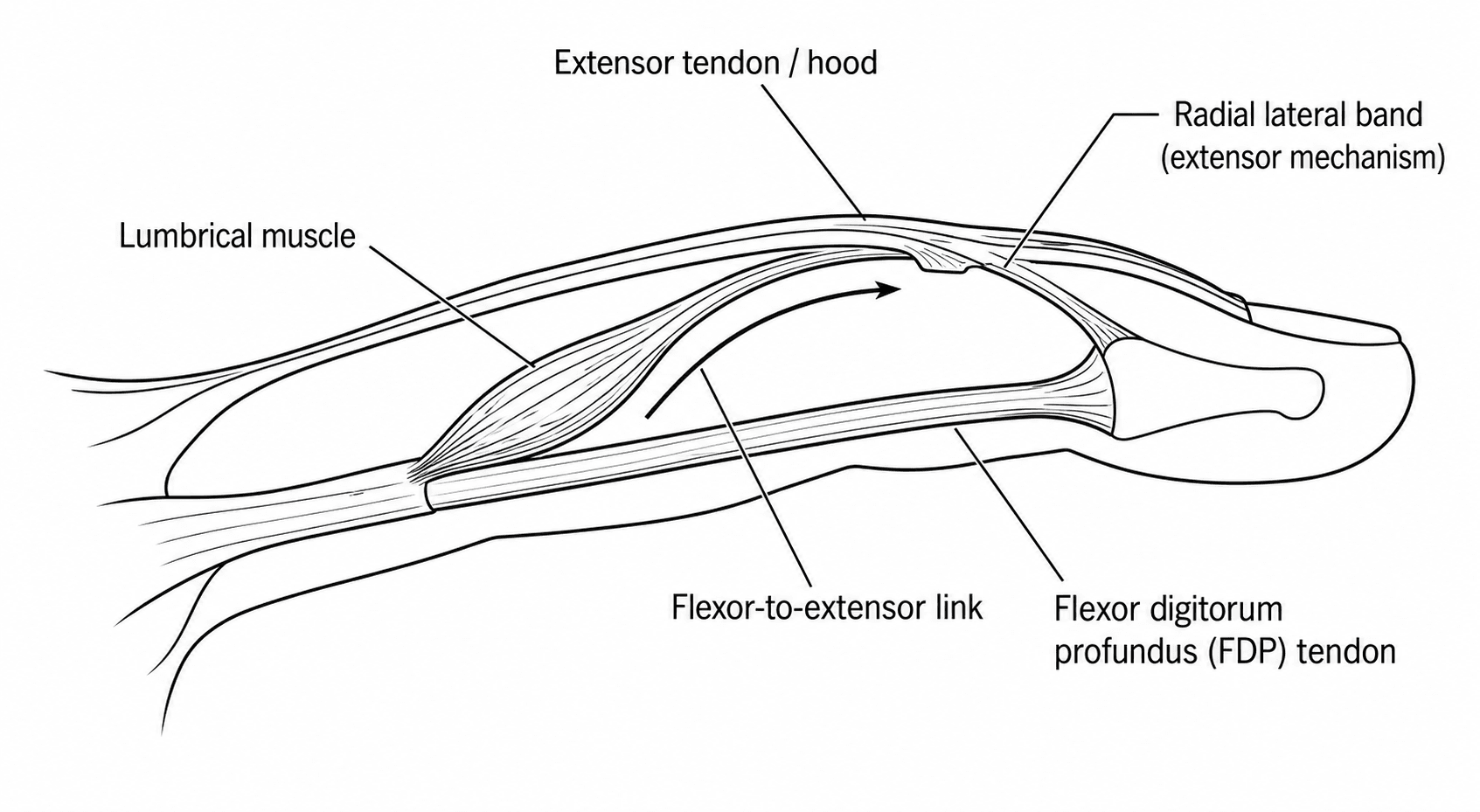
- Both phenomena stem from one piece of anatomy: the flexor digitorum profundus (FDP) tendons to the fingers arise from a SINGLE COMMON MUSCLE BELLY (so the fingers' deep flexors are not fully independent), and the LUMBRICAL muscles originate from the FDP tendons and insert into the radial lateral band of the extensor mechanism - a muscle that bridges a flexor and an extensor.
- The QUADRIGA EFFECT is loss of full active flexion and grip strength in the OTHER fingers when ONE FDP is functionally too short - over-advanced or over-tightened at repair, tethered by adhesion, or sutured too proximally to a stump after amputation; because the tendons share a common belly, the over-tight tendon 'uses up' the excursion and the neighbouring fingers cannot complete their fist (a flexion lag and weak grip).
- The LUMBRICAL-PLUS FINGER is PARADOXICAL EXTENSION of the interphalangeal joints when the patient tries to FLEX the finger; it occurs when the FDP loses effective distal pull while the lumbrical remains attached - classically after FDP division distal to the lumbrical origin, an over-LONG flexor tendon GRAFT, or a distal-finger amputation - so contraction meant to flex the digit is diverted through the lumbrical to the extensor mechanism and extends the IP joints.
- The two are, in a sense, opposite tension errors of the same system: QUADRIGA is an FDP that is too SHORT/tight (limiting the others), and LUMBRICAL-PLUS is an FDP that is too LONG/slack or has lost its distal insertion (so its force is rerouted through the lumbrical) - both are produced by getting flexor tendon length/tension wrong.
- PREVENTION is the key clinical message: in flexor tendon repair, advancement and grafting set the CORRECT TENSION and graft LENGTH (avoid over-advancing/over-tightening = quadriga; avoid an over-long/slack graft = lumbrical-plus), and at finger amputation avoid suturing the FDP under tension to the stump or letting it retract; in ray/distal amputations be aware of the imbalance these create.
- TREATMENT, when established: the quadriga is addressed by releasing the over-tight/tethered FDP (tenolysis or release of the over-advanced tendon) to restore the common belly's excursion; the lumbrical-plus finger is treated by LUMBRICAL RELEASE (dividing the offending lumbrical) or by revising the flexor GRAFT to an appropriate length - conservative measures have also been described, but lumbrical release or an appropriately tensioned FDP graft are the standard surgical solutions.
- “Shared anatomy: FDP = one common muscle belly; lumbricals run FROM the FDP tendon TO the extensor lateral band. This explains BOTH phenomena.
- “QUADRIGA = an FDP too SHORT/tight/over-advanced/amputated-proximal -> the OTHER fingers can't fully flex (weak grip, flexion lag). Named after the 4-horse chariot.
- “LUMBRICAL-PLUS = an FDP too LONG/slack/divided distal to lumbrical origin/over-long graft -> PARADOXICAL IP EXTENSION on attempted flexion. Treat with lumbrical release or correct graft length.
One FDP over-advanced, tethered or amputated-too-proximal uses up the common belly's excursion, so the other fingers cannot fully flex - weak grip, incomplete fist. Treat by releasing the over-tight/tethered tendon.
An FDP divided distal to the lumbrical, over-long graft, or distal amputation reroutes pull through the lumbrical to the extensor, so attempting to flex extends the IP joints. Treat by lumbrical release or correct graft length.
The Shared Anatomy
The FDP tendons to the index, middle, ring and little fingers arise from a single common muscle belly (the index often the most independent), so excursion is largely shared - one finger's deep flexor cannot move fully independently of the others. The lumbricals are unique: they originate from the FDP tendons in the palm and insert into the radial lateral band of the extensor mechanism, so they run from a flexor to an extensor. These two facts - shared FDP excursion and the flexor-to-extensor lumbrical - are the entire basis of the quadriga effect and the lumbrical-plus finger.
Quadriga Effect
The quadriga effect is loss of full active flexion and grip in the OTHER fingers when one FDP is functionally too short: over-advanced or over-tightened at repair, tethered by adhesion, or sutured too proximally to a stump after amputation. Because the FDP tendons share a common muscle belly, the over-tight tendon 'uses up' the excursion and the neighbouring fingers cannot complete the fist - a flexion lag and weak grip. The name comes from the Roman four-horse chariot ('quadriga'): the reins move together, so restraining one restrains all. Treatment is to release the over-tight/tethered tendon (tenolysis, or revising an over-advanced repair/amputation tension).
Lumbrical-Plus Finger
The lumbrical-plus finger (paradoxical extension, described by Parkes) is extension of the IP joints when the patient tries to flex the finger. It occurs when the FDP loses effective distal pull while the lumbrical stays attached - classically after FDP division distal to the lumbrical origin, an over-long flexor graft, or a distal-finger amputation. Contraction intended to flex the digit instead slackens/pulls the FDP proximally, transmitting force through the lumbrical to the extensor mechanism, so the IP joints extend. Treatment is lumbrical release (dividing the offending lumbrical) or revising an over-long flexor graft to the correct length; conservative techniques have also been described.
Preventing Them: the Numbers and the Rules That Are Actually Followed
"Set the correct tension" is the right principle and useless as an instruction. Three specific rules do the work, and each corresponds to one of the operations that causes these problems.
- The rule
- Do NOT advance the tendon more than about 1 cm
- What happens if it is broken
- Over-advancement shortens the FDP, producing QUADRIGA in the other fingers and a DIP flexion contracture in this one
- The rule
- Accept a graft or staged reconstruction rather than advancing beyond that limit
- What happens if it is broken
- The same shortening - the temptation to close the gap by pulling harder is exactly how quadriga is created
- The rule
- Do NOT tenodese the flexor across the gap or suture FDP to the extensor over the stump
- What happens if it is broken
- Tethering the flexor at a fixed short length restrains the common belly - QUADRIGA in the remaining fingers
- The rule
- Set the graft to the correct length rather than erring long
- What happens if it is broken
- An over-long, slack graft leaves the FDP without effective distal pull - LUMBRICAL-PLUS
Note that the amputation rule and the graft rule pull in opposite directions, which is why the two phenomena are so often confused. Fixing the flexor too short causes quadriga; leaving it with no effective distal anchor causes lumbrical-plus. After a distal amputation both are possible - tenodese it and the other fingers suffer, leave the profundus with nothing to pull on and this finger paradoxically extends - which is the reason the flexor is simply allowed to retract rather than being anchored under tension.
The 1 cm limit and the reason for it come from Flexor Tendon Repair Techniques; the amputation rule from Ray Amputation of the Hand and Foot; and the advancement-versus-graft decision in the avulsion setting from Jersey Finger.
How to Demonstrate Each One at the Bedside
Both are diagnosed by watching an active movement rather than by imaging, and each has a specific manoeuvre.
Quadriga - examine the fingers that are not complaining. Ask the patient to make a full fist. The involved digit flexes normally, or is stiff for its own reasons, while the adjacent fingers stop short. Quantify it as the distance from each fingertip to the distal palmar crease on maximal active flexion, and compare with the other hand - a persistent gap in the uninvolved fingers, with full passive flexion, is the finding. Grip strength is measurably reduced. The distinction from a stiff joint is that the deficit is active only; if the fingers cannot be passively flexed either, the problem is the joints, not the tendon.
Lumbrical-plus - watch the finger while the patient tries to make a fist. The IP joints extend as flexion is attempted, which the patient often describes as the finger "going the wrong way" or being knocked straight. It is a paradoxical movement and is unmistakable once seen. Confirmation is anatomical rather than radiological: the history contains an FDP that has lost its distal anchor - a division distal to the lumbrical origin, an over-long graft, or a distal amputation.
Neither needs imaging to diagnose. Imaging is for defining the tendon anatomy before revision surgery, not for making the diagnosis.
The Two Side by Side
- Quadriga effect
- FDP too SHORT / over-tight / tethered
- Lumbrical-plus finger
- FDP too LONG / slack / lost distal anchor
- Quadriga effect
- Over-advanced repair, adhesion, amputation stump sutured too proximal
- Lumbrical-plus finger
- FDP divided distal to lumbrical origin, over-long graft, distal amputation
- Quadriga effect
- OTHER fingers cannot fully flex (weak grip, flexion lag)
- Lumbrical-plus finger
- Affected finger's IP joints EXTEND on attempted flexion
- Quadriga effect
- Shared common muscle belly - excursion 'used up'
- Lumbrical-plus finger
- Force rerouted FDP -> lumbrical -> extensor mechanism
- Quadriga effect
- Release/tenolyse the over-tight/tethered FDP; correct tension
- Lumbrical-plus finger
- Lumbrical release or correct flexor graft length
Lumbrical Anatomy & Why the Division Level Matters
- Anatomy: there are four lumbricals. The radial two (to index and middle) are unipennate, arising from a single FDP tendon; the ulnar two (to ring and little) are bipennate, arising from two adjacent FDP tendons. Uniquely they have no bony origin - they run from a flexor tendon to the radial lateral band of the extensor mechanism - which is precisely why force can be rerouted from FDP to extensor. (The bipennate ulnar lumbricals also link adjacent FDP tendons, reinforcing the shared-excursion mechanics behind the quadriga.)
- The division-level rule: lumbrical-plus needs the lumbrical to stay attached to an FDP that has lost its distal anchor. So FDP injury/division distal to the lumbrical origin (or an over-long graft, or a distal amputation) leaves the lumbrical pulling on a now-slack/free FDP → paradoxical extension; division proximal to the lumbrical origin removes the lumbrical's drive and does not cause it. This is why the precise level matters.
(The broader intrinsic-plus and intrinsic-minus syndromes are developed in Intrinsic-Minus and Intrinsic-Plus Hand; what matters here is the lumbrical origin and the level of division that produce a lumbrical-plus finger.)
Four lumbricals: radial two unipennate (one FDP), ulnar two bipennate (two adjacent FDPs); no bony origin - flexor tendon to extensor lateral band, which is why force reroutes. Lumbrical-plus needs FDP loss distal to the lumbrical origin (or over-long graft/amputation); a proximal division does not cause it.
Prevention - Get the Tension and Length Right
- Flexor tendon repair/advancement: set the correct tension - over-advancing/over-tightening one FDP causes quadriga (limits the other fingers).
- Flexor tendon grafting: set the correct graft length - an over-long/slack graft causes lumbrical-plus (paradoxical extension); too short risks quadriga.
- Finger amputation: do not suture the FDP under tension to the stump (quadriga) and be aware that distal amputation can create a lumbrical-plus imbalance; many surgeons avoid tenodesing FDP to FDS under tension.
- Recognise early: test active flexion of all fingers (quadriga = the others lag/are weak) and watch for paradoxical IP extension on attempted flexion (lumbrical-plus).
Testing for Them at the Bedside
- Quadriga: ask the patient to make a full fist. The diagnostic finding is that the other (uninvolved) fingers cannot fully flex - an incomplete fist with a flexion lag at the PIP/DIP and weak grip - while the involved (over-tight/tethered/short) finger looks satisfactory. A useful demonstration: passively extending the involved finger slackens the common belly and improves the others' flexion, whereas flexing it worsens them.
- Lumbrical-plus: ask the patient to actively flex the finger - the IP joints paradoxically extend (with MCP flexion). The confirmatory manoeuvre is to block/hold the MCP joint (preventing MCP flexion and slackening the lumbrical): this abolishes the paradoxical extension and confirms the lumbrical is the culprit; active flexion effort exaggerates it.
The pattern distinguishes them: in quadriga the OTHER fingers under-flex (the involved finger may look normal), whereas in lumbrical-plus the SAME finger paradoxically extends on attempted flexion. (General hand examination is covered in Hand Examination and Clinical Localisation; the manoeuvres above are the phenomenon-specific ones.)
Quadriga: make a fist → the other fingers can't fully flex (passively extending the tight finger improves them). Lumbrical-plus: active flexion → the same finger's IP joints extend, and blocking the MCP (slackening the lumbrical) abolishes it - confirming the lumbrical.
Mnemonics & Memory Aids
SHORT vs LONG
Hook:SHORT FDP -> quadriga (the others can't flex); LONG/divided FDP -> lumbrical-Plus (paradoxical extension).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“After a finger amputation, a patient cannot fully make a fist with the neighbouring fingers. What has happened and why?”
“A patient with an over-long flexor tendon graft notices that when he tries to bend the finger, the tip straightens instead. Explain this.”
Shared anatomy
- FDP tendons arise from ONE common muscle belly (shared excursion)
- Lumbricals originate from FDP tendons, insert on the radial lateral band
- Both phenomena follow from this anatomy
Quadriga effect
- One FDP too SHORT/tight (over-advanced, tethered, amputated proximal)
- The OTHER fingers cannot fully flex - weak grip, flexion lag
- Treat: release/tenolyse the over-tight tendon; correct amputation tension
Lumbrical-plus finger
- FDP too LONG/slack/divided distal to lumbrical / over-long graft / distal amputation
- Paradoxical IP EXTENSION on attempted flexion (often middle finger; Parkes)
- Treat: lumbrical release or correct flexor graft length
Prevention
- Repair/advancement: correct tension (avoid over-tight = quadriga)
- Grafting: correct graft length (avoid over-long = lumbrical-plus)
- Amputation: do not suture FDP under tension to the stump
Evidence & Key Studies
Pathomechanics of lumbrical and FDP muscle tears (the quadriga effect) - a cadaveric model
- Lumbrical muscles originate on the FDP tendons; injuries occur when a shear force acts between origins on adjacent FDP tendons as they glide, and other structures of the deep flexor complex are affected via the so-called quadriga effect.
- In a cadaveric loading model of isolated 5th-finger FDP loading, rupture occurred with lumbrical detachment from the 4th FDP and changes in the FDP tendons at the distal forearm, demonstrating the shared deep-flexor mechanics underlying the quadriga effect.
- The study confirms that loading one finger's FDP transmits effects to adjacent fingers through the shared deep-flexor complex.
Lumbrical-plus (paradoxical extension) finger - description and management
- Paradoxical extension, termed the 'lumbrical-plus' finger by Parkes in 1970, is characterised by extension of the interphalangeal joints when the patient flexes the fingers, and is most common in the middle finger.
- Standard treatment involves lumbrical muscle release or a flexor digitorum profundus graft of an appropriate length.
- A conservative technique for the lumbrical-plus deformity was also described, as reports of conservative management were lacking.
The shared deep-flexor mechanics underlying the quadriga effect (lumbricals arising from the FDP tendons, effects transmitted between fingers through the common deep-flexor complex) come from the cited Carnicero cadaveric study, and the definition and treatment of the lumbrical-plus (paradoxical extension) finger - lumbrical release or an appropriately-lengthened FDP graft - from the cited Gangatharam report. The common FDP muscle-belly anatomy, the 'quadriga' analogy, and the causative tension/length errors in repair, grafting and amputation are standard, well-established teaching. The 1 cm limit on FDP advancement, and the DIP flexion contracture that accompanies over-advancement, are taken from Flexor Tendon Repair Techniques; the rule against tenodesing the flexor across an amputation gap from Ray Amputation of the Hand and Foot; and the advancement-versus-graft decision in tendon avulsion from Jersey Finger - so the four pages give the same operative instruction. (See also Flexor Tendon Lacerations and Flexor Tendon Rehabilitation.)