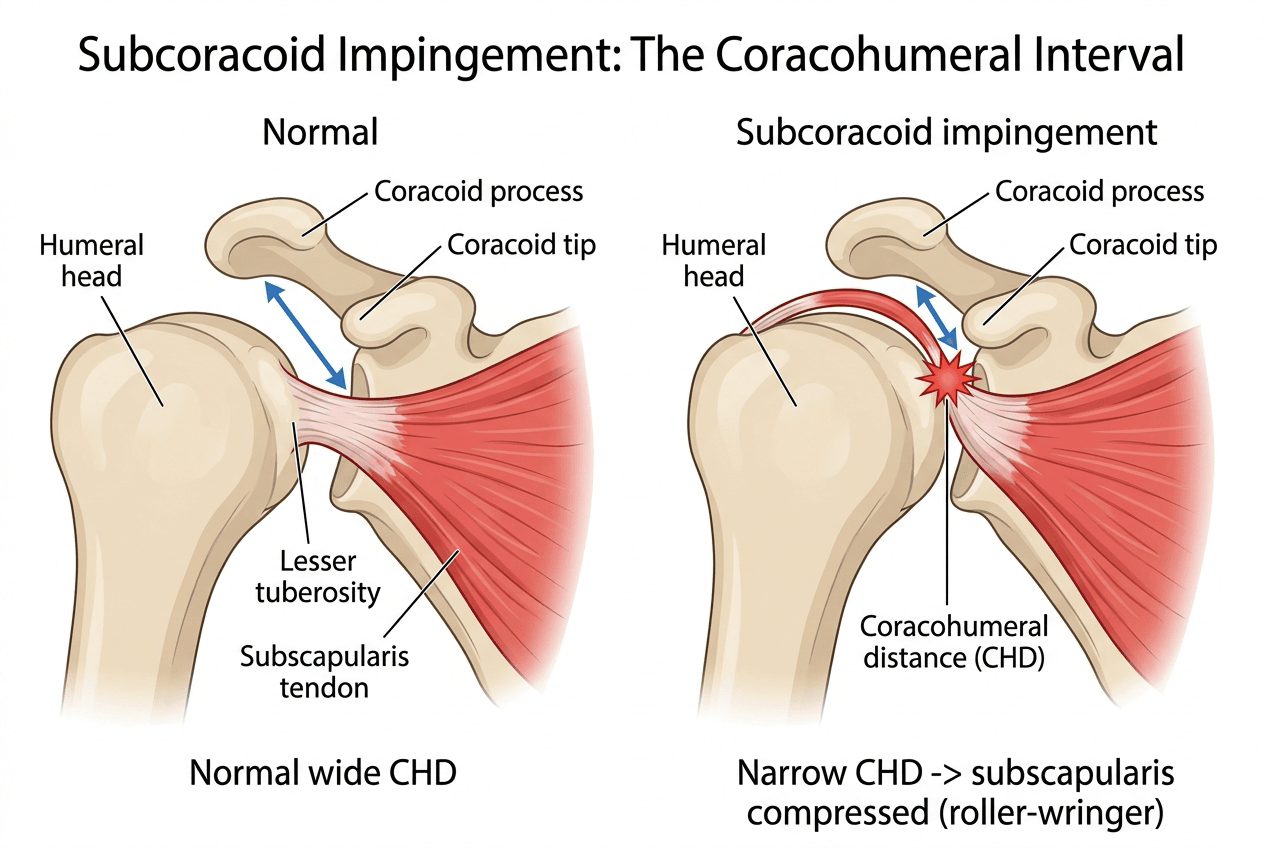
Narrowing of the Coracohumeral Interval
- Subcoracoid impingement is ANTERIOR shoulder pain arising from narrowing of the CORACOHUMERAL INTERVAL - the space between the tip of the coracoid process and the lesser tuberosity of the humerus - in which the SUBSCAPULARIS tendon is compressed (and abraded) between the coracoid and the humeral head, often described as a 'roller-wringer' effect on the tendon.
- The interval is quantified by the CORACOHUMERAL DISTANCE (CHD) on axial (and sagittal-oblique) MRI; a narrowed CHD and increased coracoid overlap define a tight subcoracoid space, and arthroscopic decompression (coracoplasty) increases the CHD and reduces coracoid overlap.
- Causes of a tight interval include a coracoid that is congenitally/developmentally too LONG or too LATERALLY placed, and IATROGENIC/post-surgical change - particularly after coracoid-transfer stabilisation (Latarjet/Bristow) or glenoid osteotomy that brings the coracoid closer to the humerus - as well as dynamic narrowing in provocative positions.
- The provocative position reproduces pain when the shoulder is brought into FORWARD FLEXION, ADDUCTION and INTERNAL ROTATION (the coracoid impingement test), which drives the lesser tuberosity towards the coracoid; pain is anterior, over the coracoid, and may be associated with subscapularis signs (a positive belly-press or lift-off if the tendon is involved).
- There is a genuine CONTROVERSY about causation: subcoracoid impingement is classically implicated in upper-border SUBSCAPULARIS tears, but comparative MRI studies have found NO significant difference in coracohumeral distance or coracoid overlap between shoulders with isolated subscapularis tears and the opposite healthy shoulders, with coracoacromial-ligament degeneration (a subacromial process) present in most - so a narrowed interval is not proven to cause the tear, and subscapularis pathology should not be attributed to it uncritically.
- THE CONTROVERSY LARGELY RESOLVES ON TWO DISTINCTIONS. First, TEAR MECHANISM: measured on axial MRI, DEGENERATIVE subscapularis tears had a mean CHD of 8.6 mm against 10.2 mm for TRAUMATIC tears and 10.4 mm for controls (p = 0.0003), with traumatic tears INDISTINGUISHABLE from controls - and a CHD below 6 mm occurred ONLY in degenerative tears. A study pooling both mechanisms will therefore find nothing. Second, WHAT IS MEASURED: an absolute CHD is weak because the normal range is wide (roughly 7-14 mm), whereas the SIDE-TO-SIDE DISCREPANCY measured bilaterally in 213 patients predicted subscapularis tears with an AUC of 0.882, a 0.5 mm cut-off giving 76.4% sensitivity and 99.3% specificity.
- CORACOID OVERLAP, though widely quoted, did NOT differ between sides in either the tear or the control group of that 213-patient bilateral study - so it does not discriminate and should not be leaned on, even though coracoplasty does reduce it. Use the patient's own contralateral shoulder as the reference rather than any published absolute value, and remember that an asymmetric interval identifies a mechanical association, not the source of the pain.
- MANAGEMENT is CONSERVATIVE first - activity/biomechanical modification, physiotherapy and corticosteroid injection - reserving ARTHROSCOPIC SUBCORACOID DECOMPRESSION (CORACOPLASTY, resecting the posterolateral coracoid to widen the interval) for recalcitrant, genuinely subcoracoid pain, often combined with addressing any subscapularis tear; coracoplasty reliably increases the CHD and improves pain and subscapularis strength in selected patients.
- “Subcoracoid impingement = anterior shoulder pain from a narrowed CORACOHUMERAL interval; subscapularis pinched between coracoid tip and lesser tuberosity ('roller-wringer').
- “Quantify with coracohumeral distance (CHD) on MRI; provocative position = forward flexion + adduction + internal rotation; causes incl. long/lateral coracoid and post-Latarjet.
- “Controversial as a cause of subscapularis tears. Conservative first; arthroscopic coracoplasty for recalcitrant cases.
- “The conflict resolves on mechanism: CHD narrowed in DEGENERATIVE tears (8.6 mm) but NORMAL in traumatic ones (10.2 vs 10.4 mm controls); under 6 mm occurred only in degenerative tears.
- “Absolute CHD is weak (normal ~7-14 mm) - the SIDE-TO-SIDE discrepancy discriminates (AUC 0.882; 0.5 mm = 76% sens, 99% spec). Coracoid overlap did NOT differ between sides.
Anterior shoulder pain reproduced by forward flexion + adduction + internal rotation; a narrowed coracohumeral distance on MRI; possible subscapularis signs.
It is implicated in subscapularis tears but not proven to cause them - don't attribute subscapularis pathology to a tight interval uncritically.
Anatomy, Mechanism & Diagnosis
Subcoracoid impingement is anterior shoulder pain from narrowing of the coracohumeral interval - the space between the coracoid tip and the lesser tuberosity - so the subscapularis tendon is compressed between the coracoid and the humeral head (the 'roller-wringer' effect). The interval is measured as the coracohumeral distance (CHD) on axial/sagittal MRI; a narrow CHD with increased coracoid overlap defines a tight space. A tight interval may be congenital/developmental (a long or laterally placed coracoid), iatrogenic (after coracoid-transfer stabilisation such as Latarjet/Bristow, or glenoid osteotomy), or dynamic. The provocative position is forward flexion, adduction and internal rotation, which drives the lesser tuberosity towards the coracoid and reproduces anterior pain, sometimes with subscapularis signs (belly-press/lift-off).
Differential of Anterior Shoulder Pain
Subcoracoid impingement is easily confused with subacromial impingement, and the broader skill is a structured differential of anterior shoulder pain and how each cause is told apart. Each is developed in full at Subacromial Impingement, Biceps Tendon Pathology, SLAP Tears, Subscapularis Tears, AC Joint Injuries, Calcific Tendinitis of the Shoulder and Anterior Shoulder Instability.
- Discriminating features
- Pain over the coracoid; provocative position forward flexion + ADDuction + internal rotation; asymmetric coracohumeral distance versus the other side
- The test that settles it
- A diagnostic subcoracoid injection that abolishes the pain - the most useful single manoeuvre
- Discriminating features
- Anterolateral pain, painful arc; a coracoacromial-arch process
- The test that settles it
- Positive Neer and Hawkins with relief after a subacromial injection - a different injection site from the above
- Discriminating features
- Pain over the bicipital groove; deep clicking with a SLAP lesion
- The test that settles it
- Speed's and O'Brien's tests; MR arthrography or arthroscopy for the labrum
- Discriminating features
- Increased passive external rotation, a positive bear-hug
- The test that settles it
- Weak belly-press and lift-off, confirmed on MRI - and remember subscapularis tearing and subcoracoid narrowing often coexist
- Discriminating features
- Pain localised to the AC joint
- The test that settles it
- Cross-body adduction (scarf) test, with an AC joint injection if still uncertain
- Discriminating features
- Acute, severe, often non-positional pain out of proportion to the examination
- The test that settles it
- A plain radiograph showing the deposit - do this before attributing severe acute pain to impingement
- Discriminating features
- Younger patient, history of dislocation or subluxation
- The test that settles it
- Apprehension and relocation tests; the history usually gives it away
Each of these is developed separately in subacromial impingement, biceps tendon pathology, SLAP tears, subscapularis tears, rotator cuff tears, AC joint injuries, calcific tendinitis of the shoulder and anterior shoulder instability.
Localise the pain and use the position: coracoid tenderness with flexion-adduction-internal-rotation = subcoracoid; anterolateral pain with a painful arc/Hawkins = subacromial; bicipital-groove pain = biceps/SLAP; AC-joint point tenderness with cross-body adduction = AC; and weakness on belly-press/ lift-off flags the subscapularis. A subcoracoid injection that abolishes the pain is the cleanest confirmation before coracoplasty.
The Causation Controversy & Management
- Be critical about causation. Subcoracoid impingement is classically implicated in upper-border subscapularis tears, but comparative MRI studies have found no significant difference in CHD or coracoid overlap between shoulders with isolated subscapularis tears and the contralateral healthy shoulder, with coracoacromial-ligament degeneration (a subacromial process) present in most - so a tight interval is not proven to cause the tear.
- Conservative management first: activity/biomechanical modification, physiotherapy, and a corticosteroid injection into the subcoracoid space (also diagnostic).
- Arthroscopic subcoracoid decompression (coracoplasty) - resecting the posterolateral coracoid to widen the interval - is reserved for recalcitrant, genuinely subcoracoid pain, often combined with repair of any subscapularis tear.
- Outcome: coracoplasty reliably increases the CHD, reduces coracoid overlap, and improves anterior pain and subscapularis strength in selected patients.
The key judgement in subcoracoid impingement is to take the diagnosis seriously as a cause of genuine anterior shoulder pain while remaining critical about its role in subscapularis tears: because comparative imaging shows that the coracohumeral distance is often no different from the healthy side and that coracoacromial (subacromial) degeneration is common, attributing a subscapularis tear solely to a 'tight' subcoracoid interval can lead to an unnecessary or insufficient operation. Confirm that pain is truly subcoracoid (anterior, provocative position, relieved by a subcoracoid injection) before offering coracoplasty, treat conservatively first, and address the subscapularis on its own merits.
Measuring the Interval: Coracohumeral Distance and Coracoid Overlap
- Coracohumeral distance (CHD). The shortest distance between the coracoid tip and the lesser tuberosity/humeral head on axial (and sagittal-oblique) MRI/CT. Published control shoulders average around 10.4 mm on MRI, with a wide normal range spanning roughly 7 to 14 mm, so no single normal value applies to everyone. A CHD below 6 mm is the usual threshold for a narrowed space, and in one series that value occurred only in shoulders with degenerative subscapularis tears. It can also narrow dynamically, so the provocative position and the symptoms matter as much as the static number.
- Coracoid overlap. How far the coracoid tip projects laterally beyond the glenoid on axial imaging. It is widely quoted, but when measured bilaterally in 213 patients it did not differ between sides in either those with or those without a subscapularis tear - so it did not discriminate, and it should not be leaned on. Coracoplasty does reduce it, alongside increasing the CHD.
- The measurement that does discriminate is the side-to-side difference. Bilateral CHD discrepancy predicted subscapularis tears with an AUC of 0.882, a 0.5 mm cut-off giving 76.4% sensitivity and 99.3% specificity - far more useful than any absolute value, because it uses the patient as their own control.
- Why imaging remains supportive rather than diagnostic. Even a genuinely asymmetric interval identifies a mechanical association, not the source of the pain - correlate with anterior pain, the provocative position and a relieving subcoracoid injection before acting on it.
Know the numbers and their limits: control shoulders average about 10.4 mm on MRI with a normal range of roughly 7-14 mm, and below 6 mm is the narrowed threshold - a value that in one series appeared only in degenerative subscapularis tears. Coracoid overlap did not differ between sides in a 213-patient bilateral study, so do not lean on it. The discriminating measurement is the side-to-side CHD discrepancy (AUC 0.882; 0.5 mm gives 76% sensitivity, 99% specificity). Even so, imaging is supportive - confirm clinically and with a subcoracoid injection.
Resolving the Controversy: It Depends What You Measure, and Which Tear
The apparently conflicting evidence on whether a tight subcoracoid space causes subscapularis tears is less contradictory than it first appears. Two distinctions do most of the reconciling.
Distinction One: Degenerative Versus Traumatic Tears
A study of 83 arthroscopically confirmed subscapularis tears against 20 controls with an intact subscapularis measured the coracohumeral distance on axial MRI:
- Mean CHD
- 8.6 +/- 2.0 mm
- Range
- 4.0 to 13.2 mm
- Mean CHD
- 10.2 +/- 2.0 mm
- Range
- 6.6 to 16.2 mm
- Mean CHD
- 10.4 +/- 1.8 mm
- Range
- 6.8 to 14.0 mm
The degenerative group had a significantly smaller interval than either the traumatic group or the controls (p = 0.0003), while the traumatic tears were indistinguishable from controls (p = 0.79). And the threshold earns its keep with a caveat that matters more than the number: a CHD below 6 mm occurred only in patients with degenerative tears. So the subcoracoid space is narrowed in the tears you would expect it to be narrowed in - attritional ones - and normal in tears caused by an injury, which is exactly what a mechanical impingement hypothesis predicts. A study that pools both mechanisms together will find no difference.
Distinction Two: Absolute Value Versus Side-to-Side Discrepancy
The second reconciliation is what is measured. A prospective study of 213 patients undergoing arthroscopic cuff repair measured the interval bilaterally on CT, comparing 72 with subscapularis tears against 141 without:
- In the tear group the affected shoulder had a significantly smaller CHD than the patient's own opposite shoulder (95% CI 6.1-7.2 mm versus 7.2-8.0 mm, p < 0.0001). In the control group there was no such side-to-side difference.
- Bilateral CHD discrepancy was the best predictor of a subscapularis tear, with an area under the curve of 0.882; a cut-off of 0.5 mm gave a sensitivity of 76.4% and a specificity of 99.3%.
- Coracoid overlap did not differ between sides in either group - so despite being widely quoted, it did not discriminate.
A single absolute CHD is a weak measurement because the normal value varies between people; the patient's own contralateral shoulder is the better reference. That is why comparisons of absolute values across different patients have been inconclusive while a within-patient comparison performs well.
Say what the evidence actually shows. CHD is narrowed in degenerative subscapularis tears (mean 8.6 mm) but normal in traumatic ones (10.2 mm, no different from controls at 10.4 mm), and a CHD below 6 mm occurred only in degenerative tears. The best single discriminator is not the absolute value but the side-to-side discrepancy (AUC 0.882; a 0.5 mm difference gives 76% sensitivity and 99% specificity), while coracoid overlap did not differ between sides at all.
A "narrow-looking" coracohumeral distance in isolation means little, because the normal range is wide - roughly 7 to 14 mm across the published control groups. Measure the contralateral shoulder and compare. A finding of asymmetric narrowing in a patient with anterior pain warrants specific intra-operative inspection of the subscapularis, and it remains the clinical picture plus a relieving subcoracoid injection - not the millimetres - that justifies a coracoplasty.
Mnemonics & Memory Aids
CORACOID
Hook:CORACOID: narrowed interval + Overlap, Roller-wringer on subscap, Anterior pain, measure CHD, On provocative position, Iatrogenic/long coracoid, Decompress if needed.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is subcoracoid impingement, and how would you assess a patient you suspect has it?”
“How would you manage subcoracoid impingement, and what does the evidence say about coracoplasty?”
Definition & mechanism
- Anterior shoulder pain from a narrowed coracohumeral interval (coracoid tip to lesser tuberosity)
- Subscapularis compressed between coracoid and humeral head ('roller-wringer')
- Quantified by coracohumeral distance (CHD) on MRI
Causes
- Long or laterally placed coracoid (congenital/developmental)
- Iatrogenic/post-surgical (coracoid transfer - Latarjet/Bristow; glenoid osteotomy)
- Dynamic narrowing in provocative positions
Assessment
- Provocative position: forward flexion + adduction + internal rotation
- Coracoid tenderness; subscapularis tests (belly-press, lift-off)
- MRI CHD/coracoid overlap; diagnostic subcoracoid injection
Controversy & management
- Implicated in subscapularis tears but not proven causal - imaging is supportive, not diagnostic
- Conservative first (modification, physio, injection)
- Arthroscopic coracoplasty for recalcitrant cases (+/- subscapularis repair)
The numbers that matter
- Controls average ~10.4 mm on MRI; normal range is wide, roughly 7-14 mm
- Degenerative subscap tears 8.6 mm vs traumatic 10.2 mm (traumatic = same as controls)
- CHD under 6 mm occurred ONLY in degenerative tears
- Side-to-side CHD discrepancy is the discriminator: AUC 0.882; 0.5 mm = 76% sens, 99% spec
- Coracoid overlap did NOT differ between sides in 213 patients - do not lean on it
- Asymmetric narrowing warrants specific intra-operative subscapularis inspection
Evidence & Key Studies
Effect of arthroscopic coracoplasty on subscapularis strength in subcoracoid impingement
- Subcoracoid impingement causes anterior shoulder pain; arthroscopic subcoracoid decompression (coracoplasty) is the preferred treatment in recalcitrant cases.
- Coracoplasty increased the coracohumeral distance and reduced coracoid overlap, with improvement in anterior pain, internal rotation, ASES score and subscapularis strength.
- The improvement in subscapularis strength was inversely related to the postoperative coracohumeral distance, indicating a mechanical effect of the coracoid on the subscapularis.
Is it subcoracoid or subacromial impingement that tears the subscapularis? An MRI comparison
- In patients with isolated subscapularis tears, coracohumeral distance and coracoid overlap did not differ significantly between the operated and the contralateral healthy shoulder.
- Coracoacromial-ligament degeneration (a subacromial process) was present in 75% of patients.
- These findings question whether subcoracoid narrowing is the true cause of isolated subscapularis tears, implicating subacromial factors instead.
The coracohumeral distance in shoulders with traumatic and degenerative subscapularis tendon tears
- Axial MRI coracohumeral distance in 83 arthroscopically confirmed subscapularis tears (44 degenerative, 39 traumatic) against 20 controls with an intact subscapularis.
- Degenerative tears had a significantly smaller CHD (8.6 +/- 2.0 mm) than traumatic tears (10.2 +/- 2.0 mm) or controls (10.4 +/- 1.8 mm), p = 0.0003; traumatic tears did not differ from controls (p = 0.79).
- A CHD of less than 6 mm occurred only in patients with degenerative subscapularis tears - so the narrowed interval tracks the attritional mechanism specifically.
Bilateral coracohumeral distance discrepancy is associated with subscapularis tear in rotator cuff rupture patients
- Bilateral CT measurement in 213 consecutive patients undergoing arthroscopic cuff repair, 72 with and 141 without a subscapularis tear.
- In the tear group the affected shoulder had a smaller CHD than the patient's own contralateral shoulder (95% CI 6.1-7.2 versus 7.2-8.0 mm, p < 0.0001); no such side-to-side difference existed in the control group, and coracoid overlap did not differ between sides in either group.
- Bilateral CHD discrepancy was the best predictor of a subscapularis tear (AUC 0.882); a 0.5 mm cut-off gave 76.4% sensitivity and 99.3% specificity, and its presence warrants specific intra-operative inspection of the subscapularis.
The description of subcoracoid impingement as a cause of anterior shoulder pain and the effect of coracoplasty - widening the interval, reducing overlap and improving subscapularis strength, with that improvement inversely related to the postoperative CHD - come from the cited Acan study. The finding that CHD and coracoid overlap do not differ from the healthy side in isolated subscapularis tears, with coracoacromial ligament degeneration in 75%, is Cetinkaya.
The reconciliation of that apparent conflict draws on two further sources. The separation by tear mechanism - degenerative 8.6 mm against traumatic 10.2 mm and controls 10.4 mm, with a CHD under 6 mm occurring only in degenerative tears - is Balke, a cohort of 83 tears and 20 controls. The bilateral measurements, the finding that coracoid overlap does not differ between sides, and the discriminating performance of side-to-side CHD discrepancy (AUC 0.882, 0.5 mm cut-off, sensitivity 76.4%, specificity 99.3%) are Zhu, in 213 patients measured on CT rather than MRI, which is worth noting because absolute values are not interchangeable between the two modalities. Reading those two alongside Cetinkaya is what suggests that pooling tear mechanisms, and comparing absolute values between different people rather than between a patient's own shoulders, explains the inconclusive results - that synthesis is an inference from the studies read together rather than a conclusion any one of them states.
No verified figure was identified for how much coracoid may safely be resected at coracoplasty before the conjoint tendon origin is compromised, so no amount is given. The coracohumeral-interval anatomy, the roller-wringer mechanism, the provocative position and the conservative-then-coracoplasty pathway are standard, well-established teaching. (See also Subscapularis Tears, Subacromial Impingement and External Impingement.)