A Reversible Bone Marrow Oedema Syndrome
- Transient osteoporosis of the hip (TOH) - a form of BONE MARROW OEDEMA SYNDROME - is a rare, IDIOPATHIC, SELF-LIMITING and REVERSIBLE cause of acute hip pain, characterised by a temporary fall in bone mineral density of the proximal femur that recovers over about 6-12 (occasionally up to 24) months.
- It classically affects two groups: MIDDLE-AGED MEN, and WOMEN in the THIRD TRIMESTER of PREGNANCY (or early post-partum); presentation is sudden/subacute groin and hip pain WORSE ON WEIGHT-BEARING with an antalgic gait and no preceding trauma. A LEFT-sided predilection is often quoted, but in the single retrospective series giving a prevalence the left-sided association was found in an entirely MALE group of about eight patients - it is not a pregnancy-specific finding and rests on a very small numerator.
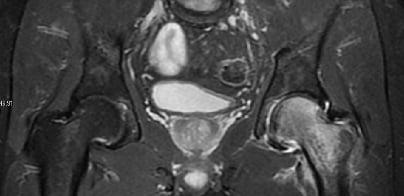
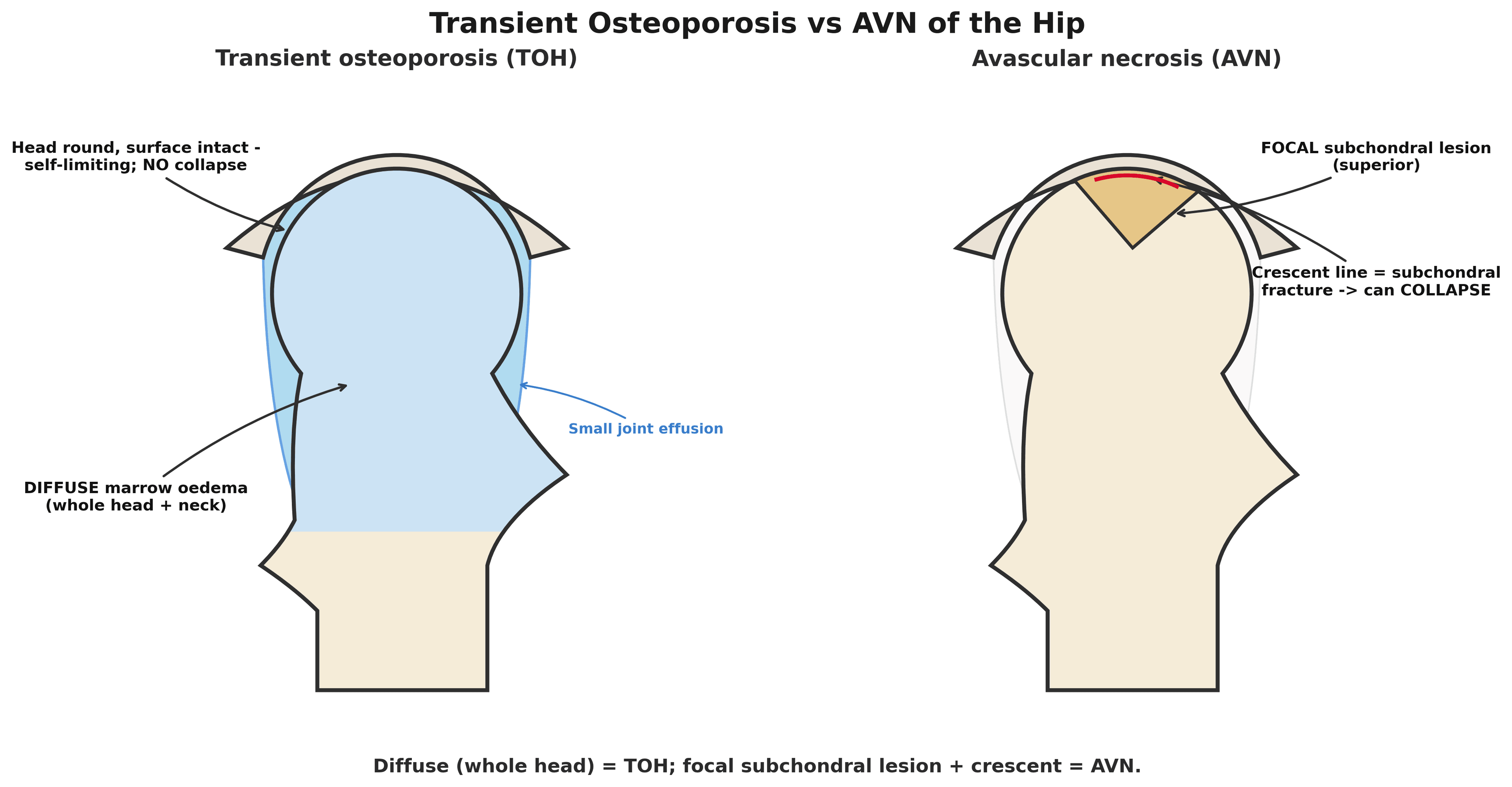
- MRI is the key test and shows DIFFUSE BONE MARROW OEDEMA of the femoral HEAD extending into the neck (low T1, high T2/STIR signal), often with a small joint effusion, but - crucially - NO focal subchondral fracture line/crescent and no segmental lesion; plain radiographs later show femoral-head osteopenia with a PRESERVED joint space and NO collapse.
- The most important differential is AVASCULAR NECROSIS (osteonecrosis): AVN is a FOCAL, segmental subchondral lesion (double-line sign, crescent sign) that can progress to COLLAPSE, whereas TOH is DIFFUSE, reversible oedema that does not - distinguishing them changes management entirely; also exclude septic/inflammatory arthritis and an occult/insufficiency fracture.
- MANAGEMENT is CONSERVATIVE: PROTECTED (reduced) WEIGHT-BEARING with crutches, analgesia, and time, because the condition self-resolves; protected weight-bearing also reduces the risk of a SUBCHONDRAL INSUFFICIENCY FRACTURE through the oedematous, weakened bone. Bisphosphonates and prostacyclin analogues (iloprost) may speed recovery, and core decompression is occasionally used in refractory cases.
- REGIONAL MIGRATORY OSTEOPOROSIS is a related entity in which the oedema and pain MIGRATE from joint to joint over time (e.g. the contralateral hip, knee or ankle); it is managed in the same conservative way.
- “TOH = self-limiting bone marrow oedema syndrome of the femoral head in middle-aged men or 3rd-trimester pregnant women. A left-sided predilection is quoted but comes from about eight all-male patients in one series - do not present it as a pregnancy finding.
- “MRI: DIFFUSE femoral-head marrow oedema, no crescent/collapse - this distinguishes it from FOCAL avascular necrosis.
- “Treat conservatively: protected weight-bearing + analgesia + time (6-12 months); protect against subchondral insufficiency fracture; +/- bisphosphonate. Migratory variant = regional migratory osteoporosis.
DIFFUSE femoral-head marrow oedema, no crescent/collapse, reversible. Treat conservatively
- it self-resolves.
FOCAL segmental subchondral lesion (double-line/crescent sign) that can progress to collapse. May need core decompression/arthroplasty - see avascular necrosis of the hip.
Why It Happens: Proposed Pathophysiology
No single cause has been established, but several mechanisms are proposed and each is examinable.
- Ischaemic / vascular. Altered local microcirculation with venous stasis and raised intraosseous pressure producing marrow oedema.
- Neurovascular (algodystrophy / CRPS-like). Regional sympathetic dysregulation with hyperaemia and accelerated bone turnover - the basis for the overlap of TOH and regional migratory osteoporosis with the complex-regional-pain-syndrome spectrum.
- Mechanical / subchondral microfracture. A subchondral stress response / insufficiency microfracture with reactive oedema - which links TOH to the subchondral-insufficiency-fracture differential.
- Pregnancy-specific contributors. Increased mechanical load, hormonal and calcium/PTH/vitamin-D changes, and proposed compression of the obturator nerve/femoral vein by the gravid uterus causing venous stasis.
- Histology (where sampled). Marrow oedema with increased osteoclastic and osteoblastic activity and NO osteonecrosis - the cellular distinction from AVN.
TOH is idiopathic, but offer the proposed mechanisms: vascular (venous stasis/raised intraosseous pressure), neurovascular/algodystrophy (CRPS-like sympathetic dysregulation - hence the overlap with regional migratory osteoporosis), and mechanical (a subchondral insufficiency microfracture with reactive oedema); in pregnancy add mechanical load + hormonal change + uterine vein/nerve compression. Histologically there is oedema and high turnover but NO necrosis - the key contrast with AVN.
Presentation & Who Gets It
TOH presents with sudden or subacute groin/hip pain that worsens on weight-bearing, producing an antalgic gait and reduced range of movement, usually with no preceding trauma. The two classic groups are middle-aged men and women in the third trimester of pregnancy (or early post-partum). It is part of the bone marrow oedema syndrome spectrum, is idiopathic, and is self-limiting, resolving over roughly 6-12 months (sometimes up to 24). Because it mimics more sinister hip pathology, the diagnosis hinges on recognising the typical patient and the characteristic MRI.
Imaging & Diagnosis
- MRI (diagnostic): diffuse bone marrow oedema of the femoral head extending into the neck - low T1, high T2/STIR signal - often with a small joint effusion, and importantly NO focal subchondral fracture line/crescent and no segmental necrotic lesion.
- Radiographs: initially normal, then (after a few weeks) osteopenia of the femoral head/neck with a preserved joint space and no collapse.
- Exclude the differentials: AVN (focal subchondral lesion, double-line/crescent sign), septic/ inflammatory arthritis (aspirate/bloods if suspected), and an occult or subchondral insufficiency fracture; bone densitometry may show transient regional bone loss.
- Diagnosis is essentially clinical + MRI; biopsy is not routine.
The Bone Marrow Oedema Spectrum and Its Differential
Several conditions across the bone-marrow-oedema syndrome spectrum share marrow oedema on MRI and must be separated from TOH, including subchondral insufficiency fracture.
- Distinguishing feature
- DIFFUSE oedema of head/neck, NO focal lesion/line, reversible; classic demographics (middle-aged man / late-pregnancy woman)
- What settles it
- MRI pattern plus resolution on follow-up imaging
- Distinguishing feature
- The same self-limiting oedema MIGRATING between joints over time
- What settles it
- The migratory history itself - do not re-investigate each joint from scratch
- Distinguishing feature
- A FOCAL segmental subchondral lesion (double-line/crescent); oedema may herald it - so it can mimic TOH
- What settles it
- Repeat MRI: TOH resolves, AVN declares a focal lesion
- Distinguishing feature
- A low-signal SUBCHONDRAL LINE on the oedema background (older/osteoporotic); a cause or complication of BMES
- What settles it
- Look for the line specifically on T1 and on fluid-sensitive sequences
- Distinguishing feature
- Raised CRP/ESR/WCC, effusion
- What settles it
- Aspirate if suspected - the one diagnosis here that cannot wait
- Distinguishing feature
- Regional pain with autonomic/trophic changes; overlaps the BME spectrum
- What settles it
- Clinical - autonomic and trophic signs, not the MRI
Each of these is developed separately in avascular necrosis of the hip, femoral neck stress fractures, septic arthritis pathophysiology, complex regional pain syndrome and, for the imaging of marrow signal in general, MRI bone marrow signal.
TOH sits in the bone marrow oedema syndrome spectrum with regional migratory osteoporosis. Separate it from a subchondral insufficiency fracture (low-signal subchondral line), early AVN (focal lesion/ double-line - and because AVN can start as oedema, follow up to confirm resolution), infection (raised markers) and CRPS. The TOH signature remains diffuse, line-free, reversible oedema in the classic patient.
How Solid Are the Numbers - and Does It Always Resolve on Its Own?
Calling transient osteoporosis self-limiting is correct as a general statement, and most patients do settle with protection and time. It should not, however, be delivered as a promise that nothing further will be needed. In a reported case of bilateral pregnancy-related disease, rest and paracetamol did not improve the patient at all; her symptoms persisted through delivery and into lactation, the diagnosis was only made late, during breastfeeding, and remission followed three months after starting a bisphosphonate once breastfeeding stopped. That is a single case and cannot give a failure rate, but it makes two practical points that a confident "it resolves by itself" obscures: the pregnant patient's hip pain is easily attributed to the pregnancy and the diagnosis is frequently delayed, and failure to improve is not a reason to doubt the diagnosis - it is a reason to reconsider pharmacological treatment once it is safe to give. Set a review date rather than discharging on reassurance alone.
Know the strength of the evidence you are quoting. The often-cited prevalence of 2.5 percent among patients having hip MRI for hip pain comes from 314 patients at a single tertiary centre, which means the condition itself was found in only about eight people - and every "risk factor" derived from that series (age 41 to 50, left-sided pain) rests on those eight. All of them were male, so the series says nothing about the pregnancy-associated form at all. Quote it as a rough indication that the condition is uncommon, not as epidemiology.
Management
- Protected (reduced) weight-bearing with crutches until symptoms settle - this both relieves pain and protects the weakened, oedematous femoral head from a subchondral insufficiency fracture.
- Analgesia (and physiotherapy as pain allows); reassurance that the condition is self-limiting.
- Pharmacological adjuncts: bisphosphonates and prostacyclin analogues (iloprost) may accelerate resolution of the oedema and symptoms (note: bisphosphonates are avoided in pregnancy/breastfeeding).
- Refractory cases: core decompression of the femoral head can give rapid pain relief and is occasionally used (it can also help exclude early AVN).
- In pregnancy: rest, analgesia and protected weight-bearing, with bisphosphonates deferred until after delivery/breastfeeding; coordinate with obstetrics.
- Regional migratory osteoporosis: treat each affected joint the same conservative way as the oedema migrates.
The two pitfalls are (1) allowing full weight-bearing through an oedematous, demineralised femoral head, which risks a subchondral insufficiency fracture and collapse, and (2) mislabelling TOH as AVN (or vice versa) - they look superficially similar but TOH is diffuse and reversible while AVN is focal and potentially progressive. Protect weight-bearing, image with MRI, and follow up to confirm resolution.
Mnemonics & Memory Aids
TRANSIENT
Hook:TRANSIENT - reversible, diffuse oedema, protect weight-bearing.
DIFFUSE vs FOCAL
Hook:Diffuse = TOH; Focal = AVN.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old man (or a woman in late pregnancy) has acute hip pain worse on weight-bearing with no trauma. The MRI shows diffuse femoral head oedema. What is the diagnosis and how do you manage it?”
“Why must you protect weight-bearing in transient osteoporosis, and what is regional migratory osteoporosis?”
Who / presentation
- Middle-aged men; women in 3rd trimester (left-sided predilection rests on ~8 all-male patients)
- Acute atraumatic groin/hip pain, worse on weight-bearing
- Self-limiting over ~6-12 (up to 24) months
Imaging
- MRI: DIFFUSE femoral head/neck marrow oedema (low T1, high T2/STIR) + small effusion
- NO subchondral crescent/collapse (vs AVN); radiographs later show osteopenia, preserved joint space
- Exclude AVN, septic/inflammatory arthritis, insufficiency fracture
Management
- Protected (reduced) weight-bearing + analgesia + time
- Protect against subchondral insufficiency fracture
- +/- bisphosphonate / iloprost (avoid bisphosphonate in pregnancy); core decompression if refractory
Variant
- Regional migratory osteoporosis: oedema/pain migrates between joints
- Same self-limiting bone marrow oedema spectrum
- Same conservative management
Evidence & Key Studies
Prevalence of transient osteoporosis of the hip among patients with hip pain
- Transient osteoporosis of the hip (acute bone marrow oedema syndrome) is a rare condition with reduced proximal-femur bone mineral density that resolves with conservative management over 6-24 months.
- Retrospective single-centre review of 314 patients over 14 years old having hip MRI for hip pain at one tertiary hospital in Saudi Arabia, 2016 to 2019.
- Prevalence of transient osteoporosis was 2.5 percent - that is roughly EIGHT patients, on which every subsequent finding rests.
- ALL of those patients were male; half were over 40, 50 percent had left-sided pain and 75 percent a small joint effusion. The femoral head was the most affected part.
- Left-sided pain (p = 0.023) and age 41 to 50 (p = 0.012) were the associations reported - derived from that same handful of patients, so they are hypothesis-generating at best.
- For context on how non-specific hip pain is, the commonest single cause in the whole cohort was gluteus medius tendonitis (12.9 percent) and a third of patients had normal examination and investigations.
- The authors themselves state the prevalence requires confirmation by studies with a more robust design; the all-male cohort means it cannot speak to pregnancy-related disease.
Bilateral transient pregnancy-related osteoporosis of the hip: a rare presentation and mini-review
- Single case report: a 31-year-old primigravida admitted at 35 weeks with lumbar and hip pain, no history of trauma, whose pain progressed to severe movement limitation.
- BILATERAL involvement - rarer still than the usual unilateral presentation.
- Rest and paracetamol did NOT improve her; symptoms persisted through delivery and the diagnosis was only established by MRI LATE, during the lactation period.
- Bisphosphonate started once breastfeeding was discontinued produced definitive remission of symptoms three months later.
- A single case cannot give a failure rate for conservative treatment, but it shows that non-response does not refute the diagnosis and that delayed diagnosis in pregnancy is a real pattern.
The description as a self-limiting bone marrow oedema syndrome resolving over 6-24 months, the low prevalence among hip-pain patients and the reported associations come from the cited Aldhilan study - a retrospective, single-centre review in which the condition was identified in only about eight patients, all male, so its laterality and age associations are hypothesis-generating and say nothing about the pregnancy-related form. The delayed diagnosis in pregnancy, the failure of rest and simple analgesia and the bisphosphonate response after breastfeeding stopped come from the cited Thanasa report, which is a single case. The MRI distinction from AVN and conservative protected-weight-bearing management are standard, well-established teaching. No randomised trial of bisphosphonate or iloprost in this condition was retrieved, and no disease-specific dose or duration was found for either, so none is quoted - prescribe to local formulary. No published figure was retrieved for how often conservative management fails or for the incidence of subchondral insufficiency fracture in untreated disease, so the recommendation to protect weight-bearing is given on mechanical reasoning rather than a measured risk. See also avascular necrosis of the hip, osteoporosis, MRI bone marrow signal and complex regional pain syndrome.