Intra-articular Hindfoot Injuries with a Precarious Blood Supply
- A talar BODY fracture is an intra-articular fracture of the body of the talus that, unlike a talar NECK fracture, disrupts BOTH the tibiotalar (ankle) AND the subtalar (posterior facet) articular surfaces - so anatomic reduction of the joint surfaces is the priority and post-traumatic arthritis of both joints is common.
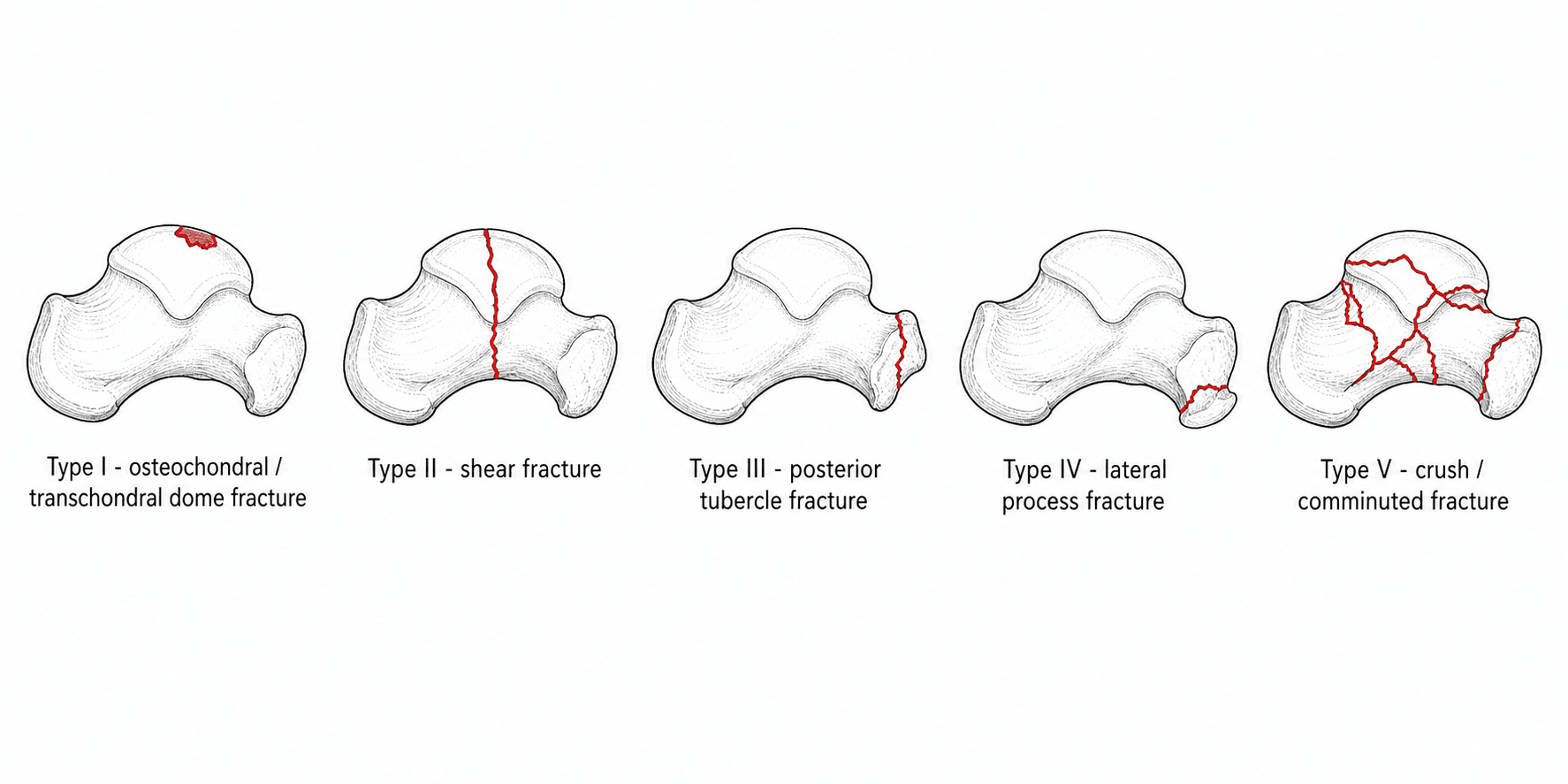
- Fractures are described by the SNEPPEN classification: I osteochondral/transchondral dome, II coronal/sagittal/horizontal SHEAR (the main body fracture), III posterior tubercle, IV lateral process, V crush/comminuted. Lateral process, posterior process and osteochondral dome lesions each have a dedicated OrthoVellum topic.
- The talus has NO muscular attachments and is largely covered by articular cartilage, so its blood supply enters through a limited non-articular area and runs largely RETROGRADE (artery of the tarsal canal from the posterior tibial, deltoid branches, and the artery of the sinus tarsi from the dorsalis pedis/peroneal). Displaced body fractures therefore carry a HIGH risk of AVASCULAR NECROSIS.
- CT is MANDATORY: plain radiographs underestimate talar body fractures, and CT defines fracture planes, articular comminution, displacement and associated injuries to plan the approach and fixation.
- Treatment of a displaced talar body fracture is ANATOMIC reduction of the articular surfaces and RIGID internal fixation (lag screws +/- mini-fragment plates); adequate exposure of the body usually requires a MEDIAL or LATERAL MALLEOLAR OSTEOTOMY, taking care to preserve the deltoid (and its blood supply). Truly non-displaced fractures may be treated non-operatively in a non-weight-bearing cast with close radiographic surveillance.
- SEPARATE THE TWO MEANINGS OF 'URGENT'. A DISLOCATED, EXTRUDED OR OPEN talus is an EMERGENCY - but because of the SKIN and the posterior tibial NEUROVASCULAR BUNDLE, not because of a clock running on osteonecrosis. For the CLOSED displaced fracture, definitive fixation can be STAGED until the soft tissues settle: in 26 displaced fractures isolated to the talus followed a mean of 74 months, a delay in surgical fixation did NOT affect outcome, union or the prevalence of osteonecrosis, and all closed displaced fractures healed regardless of the delay (union 88%). Operating through swollen, blistered skin trades a tolerable wait for a wound catastrophe.
- ARTHRITIS, NOT OSTEONECROSIS, IS THE COMMONER OUTCOME, which is the opposite of where most discussion sits. In that series post-traumatic SUBTALAR arthritis was the most common finding and occurred in EVERY patient, with 16 having more than one joint involved, while osteonecrosis affected 13 of 26; a separate series of 42 talar neck and body fractures found arthritis 23.8% against osteonecrosis 14.3%. Counsel accordingly - post-traumatic arthritis and chronic pain are EXPECTED even after anatomic reduction and stable fixation, especially after an OPEN injury (osteonecrosis followed 6 of 7 open fractures).
- Complications are frequent: POST-TRAUMATIC ARTHRITIS of the subtalar and tibiotalar joints (the commonest), AVASCULAR NECROSIS (watch for the Hawkins sign - subchondral lucency at 6-8 weeks indicating revascularisation; its ABSENCE is concerning but not diagnostic), malunion, and wound problems - these injuries are best managed at, or referred to, a foot-and-ankle/trauma centre.
- “Talar BODY fracture = intra-articular, involves BOTH tibiotalar and subtalar surfaces (vs neck fracture); Sneppen classification.
- “Retrograde blood supply (artery of tarsal canal etc.) -> high AVN risk; Hawkins sign (subchondral lucency ~6-8 wks) = revascularising; absent = AVN likely.
- “CT mandatory; displaced -> anatomic ORIF, usually needing a malleolar osteotomy for exposure.
- “'Urgent' means the DISLOCATION, not the fixation: emergency reduction for a dislocated/extruded/open talus (skin + neurovascular bundle), but delay to definitive ORIF did NOT affect union, outcome or osteonecrosis (26 fractures, 74-month follow-up, union 88%).
- “Counsel arthritis FIRST: subtalar arthritis occurred in EVERY patient in that series vs osteonecrosis in 13 of 26; arthritis and chronic pain are expected even after anatomic reduction.
Intra-articular through the body; disrupts both the tibiotalar and the subtalar (posterior facet) surfaces. Sneppen classification. Priority = anatomic articular reduction; both joints at risk of arthritis.
Extra-articular to the ankle (involves subtalar); Hawkins classification; AVN risk rises with displacement/dislocation. (See Talus Fractures.)
What Is Urgent, What Is Not, and Which Complication Actually Dominates
Urgency Belongs to the Dislocation, Not to the Fixation
The instinct that every hour of delay to definitive fixation worsens osteonecrosis does not survive the data. In 26 displaced fractures isolated to the talus - neck and body - treated by open reduction and stable fixation and followed for a mean of 74 months, a delay in surgical fixation did not appear to affect outcome, union or the prevalence of osteonecrosis, and all closed displaced fractures healed regardless of the time to surgery. The overall union rate was 88%.
That splits the word "urgent" into two different things:
- Timing
- EMERGENCY reduction
- Why
- The threat is to the skin and the posterior tibial neurovascular bundle, not to a clock running on osteonecrosis
- Timing
- STAGE the definitive fixation
- Why
- Delay did not affect union, outcome or osteonecrosis - whereas operating through compromised skin causes wound failure
- Timing
- Definitive ORIF on a planned list
- Why
- Anatomic articular reduction, done well, matters more than done fast
The distinction matters because the two errors are opposite: leaving a dislocated talus unreduced overnight risks the skin and the neurovascular bundle, while rushing a swollen, blistered ankle to definitive fixation risks a wound catastrophe in an injury that would have tolerated waiting.
Arthritis, Not Osteonecrosis, Is the Commoner Outcome
Osteonecrosis is the complication that dominates discussion of this injury, but it is not the one most patients get. In that same series, post-traumatic subtalar arthritis was the most common finding and was present in every patient, with 16 having more than one joint involved, while osteonecrosis occurred in 13 of the 26 fractures. A separate series of 42 surgically treated talar neck and body fractures found the same ordering - arthritis 23.8% against osteonecrosis 14.3%.
Both point the same way, and the counselling line follows from it: a patient with a displaced talar fracture should be told that post-traumatic arthritis and chronic pain are expected outcomes even after anatomic reduction and stable fixation, and that this is especially true after an open injury - osteonecrosis followed 6 of 7 open fractures in the cited series.
Do not conflate reducing a dislocation with fixing a fracture. The dislocated, extruded or open talus is a genuine emergency because of the skin and the neurovascular bundle. The closed displaced fracture is not - delay did not change union, outcome or osteonecrosis - so let the soft tissues settle rather than operating through blisters. And when counselling, lead with arthritis, which every patient in the cited series developed, rather than with osteonecrosis, which affected half.
Anatomy, Blood Supply & Why AVN Happens
About 60% of the talus is covered by articular cartilage and it has no muscular or tendinous attachments, so blood can only enter through the limited non-articular surfaces. The supply comes mainly from the artery of the tarsal canal (a branch of the posterior tibial artery) which is the dominant supply to the body, supplemented by deltoid branches (medially) and the artery of the sinus tarsi (from the dorsalis pedis and peroneal arteries). Much of this flow runs retrograde (distal to proximal) into the body, so a displaced body fracture readily strips the supply and causes avascular necrosis. This is the anatomical reason talar body and neck fractures behave so differently from most other fractures.
Assessment & Imaging
Talar body fractures follow high-energy mechanisms (falls from height, motor-vehicle crashes, axial loading) and are frequently part of a polytrauma or associated with other hindfoot/malleolar injuries, so a careful soft-tissue and neurovascular assessment is essential. Plain AP, lateral and mortise radiographs underestimate these fractures; CT is mandatory to define the fracture planes, the degree of articular comminution and displacement, and any associated lateral/posterior process or malleolar fractures - which together determine the surgical approach and fixation strategy.

Management
- Non-displaced fractures: a truly non-displaced talar body fracture (confirmed on CT) can be managed non-operatively in a non-weight-bearing cast/boot with close radiographic surveillance, because even minimally displaced intra-articular fractures may need fixation.
- Displaced fractures: require anatomic reduction of the articular surfaces and rigid internal fixation with lag screws, often supplemented by mini-fragment plates for comminution. Timing is dictated by the soft tissues and by whether anything is dislocated, not by a clock on osteonecrosis - delay to definitive fixation has not been shown to change union, outcome or osteonecrosis in a closed injury. Buried/headless screws are used where they would otherwise be prominent in the articular surface.
- Exposure: the body of the talus is deep and largely articular, so adequate visualisation usually requires a medial or lateral MALLEOLAR OSTEOTOMY (e.g. a medial malleolar osteotomy reflected on the deltoid ligament, preserving the deltoid blood supply to the body). The osteotomy is then fixed.
- Severe comminution (Sneppen V): anatomic reconstruction may be impossible; options include limited fixation, primary or delayed arthrodesis (tibiotalar or tibiotalocalcaneal), with the patient counselled about stiffness and AVN.
These are high-energy injuries: soft-tissue swelling and fracture blisters often dictate timing (definitive fixation may be staged after temporary stabilisation), an open fracture or an irreducible dislocation demands emergency treatment, and the surgeon must protect the deltoid ligament and its branches during a medial malleolar osteotomy, since stripping it removes one of the few remaining sources of blood to the body and worsens the risk of AVN. Complex hindfoot injuries are best referred to a foot-and-ankle/trauma centre.
Complications & Outcomes
- Avascular necrosis is the feared complication of displaced body fractures (because of the retrograde supply). The Hawkins sign - a subchondral lucency in the talar dome seen at about 6-8 weeks - reflects subchondral bone resorption that requires intact vascularity, so its presence is reassuring (revascularisation) and its absence raises concern for AVN (MRI clarifies). Not all AVN collapses; AVN without dome collapse may remain functional.
- Post-traumatic arthritis of the tibiotalar and/or subtalar joints is common after these double-articular injuries and is the main long-term outcome determinant; salvage is by arthrodesis of the affected joint(s).
- Other complications: malunion (altered hindfoot mechanics), non-union, wound problems/infection, and stiffness. Overall functional outcome correlates with the severity of the original fracture and the quality of articular reduction.
Diagnosing & Managing Avascular Necrosis
- The Hawkins sign explained. A thin subchondral lucency in the talar dome on a mortise radiograph at about 6 to 8 weeks is produced by subchondral bone resorption (disuse osteopenia), which can only occur if the bone is vascularised - so a positive sign means the talus is perfused and AVN is unlikely, while absence is concerning but not diagnostic (a still-immobilised, non-weight-bearing limb may not resorb).
- Confirming AVN. Where the Hawkins sign is absent or equivocal, MRI is the definitive test for the presence and extent of necrosis (CT shows established collapse); follow with serial imaging.
- Weight-bearing. Whether prolonged non-weight-bearing protects a necrotic talus from collapse is debated
- the historical practice of strict offloading until revascularisation has weak evidence that it prevents collapse, and many now allow protected weight-bearing once the fracture has united, individualised to the patient.
- The salvage ladder. Non-collapsed AVN can remain functional and is observed; once there is dome collapse or post-traumatic arthritis, salvage is by arthrodesis of the affected joint(s) - tibiotalar, subtalar or tibiotalocalcaneal - sometimes with bone graft to restore height; talar AVN with extensive collapse is a difficult problem and may need a combined fusion. (Hip/shoulder osteonecrosis pathophysiology is developed elsewhere; hindfoot fusions in Ankle Arthrodesis and Subtalar Arthrodesis.)
The Hawkins sign (subchondral lucency at ~6 to 8 weeks) needs intact vascularity to form, so present = perfused/reassuring, absent = concerning but not diagnostic - confirm with MRI. Prolonged non-weight-bearing has weak evidence for preventing collapse; non-collapsed AVN is observed, while collapse/arthritis is salvaged by arthrodesis (tibiotalar/subtalar/TTC).
Associated Injuries & the Extruded Talar Body
- Look for the partners. A talar body fracture is frequently accompanied by an ipsilateral medial malleolar fracture (as in the cited Moger case), a lateral or posterior process fracture, a calcaneal or navicular fracture, subtalar or total talar dislocation, and (as a high-energy axial injury) ipsilateral lower-limb and spine fractures - so image the whole foot/ankle and survey the patient.
- The extruded body - a surgical emergency. A displaced body fragment can extrude posteromedially, where it tents or breaches the skin and threatens the posterior tibial neurovascular bundle behind the medial malleolus; this needs urgent reduction to relieve skin and neurovascular pressure (an irreducible or open extrusion goes straight to theatre).
- The totally extruded ("missing") talus. Complete extrusion of the talus is a devastating open injury; current practice favours thorough debridement and reimplantation of the talus (even when fully extruded) with antibiotics rather than primary excision, accepting the high risk of AVN and infection, because primary talectomy leaves a very poor hindfoot - though some grossly contaminated cases still require excision and later reconstruction/arthrodesis.
- Open fractures follow the usual urgent debridement, antibiotic and (often staged) fixation principles, with soft-tissue cover as needed. (See Subtalar Dislocations and Total Talar Dislocation.)
Don't view the body fracture in isolation: hunt for an ipsilateral medial malleolus, process, calcaneal, navicular and subtalar/total talar dislocation, plus axial-load injuries. A posteromedially extruded body threatens the skin and posterior tibial neurovascular bundle - reduce it urgently; a totally extruded talus is generally debrided and reimplanted (not primarily excised) despite the high AVN/infection risk.
Mnemonics & Memory Aids
DSPLC
Hook:Sneppen I-V = Dome, Shear, Posterior tubercle, Lateral process, Crush.
TALUS
Hook:TALUS body fracture = two joints, AVN, lag screws, urgent reduction of a dislocation, Sneppen + CT.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How does a talar body fracture differ from a talar neck fracture, how are body fractures classified, and why are they prone to avascular necrosis?”
“A young man falls from a height and CT shows a displaced shear (Sneppen II) fracture of the talar body with intact skin. How would you manage him and what complications would you counsel him about?”
Definition & classification
- Intra-articular body fracture - disrupts tibiotalar AND subtalar surfaces
- Sneppen: I dome, II shear, III posterior tubercle, IV lateral process, V crush
- Lateral process / posterior process / OCD have dedicated topics
Blood supply & AVN
- No muscle attachments; ~60% cartilage; retrograde supply
- Artery of tarsal canal (post. tibial) dominant + deltoid + sinus tarsi (DP/peroneal)
- Hawkins sign (subchondral lucency ~6-8 wks) present = revascularising; absent = AVN
Imaging & management
- CT mandatory (plain films underestimate)
- Non-displaced: NWB cast + surveillance | Displaced: anatomic ORIF
- Exposure usually via malleolar osteotomy (protect deltoid); lag/headless screws +/- plate
Timing - two different urgencies
- EMERGENCY: dislocated, extruded or open talus (threatens skin + posterior tibial bundle)
- STAGE definitive ORIF if swollen/blistered - delay did NOT affect union, outcome or osteonecrosis
- 26 displaced talar fractures, 74-month follow-up: union 88%, all closed ones healed despite delay
Complications
- Post-traumatic SUBTALAR arthritis is the commonest - every patient in the cited series
- Osteonecrosis 13 of 26 overall; 6 of 7 OPEN fractures
- A separate 42-patient series: arthritis 23.8% vs osteonecrosis 14.3%
- Counsel that arthritis and chronic pain are EXPECTED even after anatomic reduction
- Malunion, non-union, wound problems, stiffness; salvage = arthrodesis
Evidence & Key Studies
Surgical management of talus fractures: mid-term functional and radiographic outcomes
- In a prospective series of 42 surgically treated talar neck and body fractures, 28.5% were ISOLATED talar BODY fractures (a further 21.5% combined neck-and-body), classified by Hawkins, Sneppen and Marti.
- Avascular necrosis affected the talar body in 14.3% (three requiring secondary arthrodesis) and arthritis developed in 23.8%; AVN incidence without dome collapse did not necessarily cause functional impairment.
- Functional/radiographic outcome correlated with fracture severity; osteosynthesis was advocated even for non-displaced patterns, with staged treatment for dislocated/open injuries and referral of complex injuries to foot-surgery centres.
Combined talus fracture with medial malleolar fracture: a case report with review of literature
- Describes a Sneppen type II talar body fracture with an ipsilateral medial malleolar fracture - illustrating the association of body fractures with malleolar injury and the value of the Sneppen classification.
- Treatment was open anatomic reduction of the talar body with a Herbert (headless) screw and cannulated-screw fixation of the medial malleolus.
- Emphasises early diagnosis and fixation to optimise outcome, while noting the unpredictable risks of AVN, wound complications and post-traumatic ankle arthritis.
Open reduction and stable fixation of isolated, displaced talar neck and body fractures
- Twenty-five patients with 26 displaced fractures isolated to the talus (neck and/or body) treated by open reduction and stable internal fixation, followed for a minimum of 48 and a mean of 74 months; overall union rate 88%.
- A delay in surgical fixation did not appear to affect outcome, union or the prevalence of osteonecrosis, and all closed displaced fractures healed regardless of the delay to surgery.
- Post-traumatic subtalar arthritis was the most common finding and occurred in every patient, 16 with more than one joint involved, while osteonecrosis was seen after 13 of the 26 fractures and after 6 of the 7 open fractures - so patients should be counselled that arthritis and chronic pain are expected even after anatomic reduction and stable fixation.
The proportion of body fractures and the osteonecrosis and arthritis rates of 14.3% and 23.8% come from the cited Kopp series of 42 surgically treated talar neck and body fractures, and the Sneppen-type-II body-with-malleolar example and fixation principles from the cited Moger case report, which is a single case.
The finding that delay to definitive fixation did not affect outcome, union or osteonecrosis, the 88% union rate, and the ordering of complications - subtalar arthritis in every patient against osteonecrosis in 13 of 26, and 6 of 7 open fractures - are the cited Lindvall series, which pooled displaced neck and body fractures rather than reporting body fractures separately, and is retrospective with 26 fractures. The same paper is the source of the counselling line that arthritis and chronic pain are expected outcomes even after anatomic reduction. Separating the emergency reduction of a dislocated or extruded talus from the schedulable definitive fixation of a closed one is the reading that follows from those findings placed beside the soft-tissue principle, rather than a distinction the paper draws in those words.
The Sneppen classification, the retrograde talar blood supply and the Hawkins sign are standard, well-established teaching. (See also Talus Fractures, Lateral Process Talus Fractures, Posterior Process Talus Fractures and Osteochondral Lesion of the Talus.)