Cellular & Molecular Biology for Orthopaedics
- Transcription vs translation. Transcription = DNA to RNA (nucleus); translation = RNA to protein (ribosome) — don't swap them.
- Forgetting vitamin C. Prolyl/lysyl hydroxylation of collagen needs vitamin C — its lack (scurvy) impairs collagen, causing bleeding and poor healing. This is the favourite single-fact pull.
- Cross-linking enzyme. Collagen fibrils are cross-linked by lysyl oxidase (a copper-dependent enzyme) — not by hydroxylation.
- Collagen type mix-ups. Type I = bone/tendon/skin (defective in OI); type II = hyaline cartilage; type III = early healing; type X = hypertrophic physis.
- Apoptosis is NOT inflammatory. Apoptosis is programmed, ATP-dependent and non-inflammatory (caspases, apoptotic bodies cleared by phagocytes); necrosis is the passive, swelling, inflammatory opposite (osteonecrosis, infarction).
- Naming the guardian. p53 = "guardian of the genome" (arrests the cycle / triggers apoptosis on DNA damage); loss drives oncogenesis.
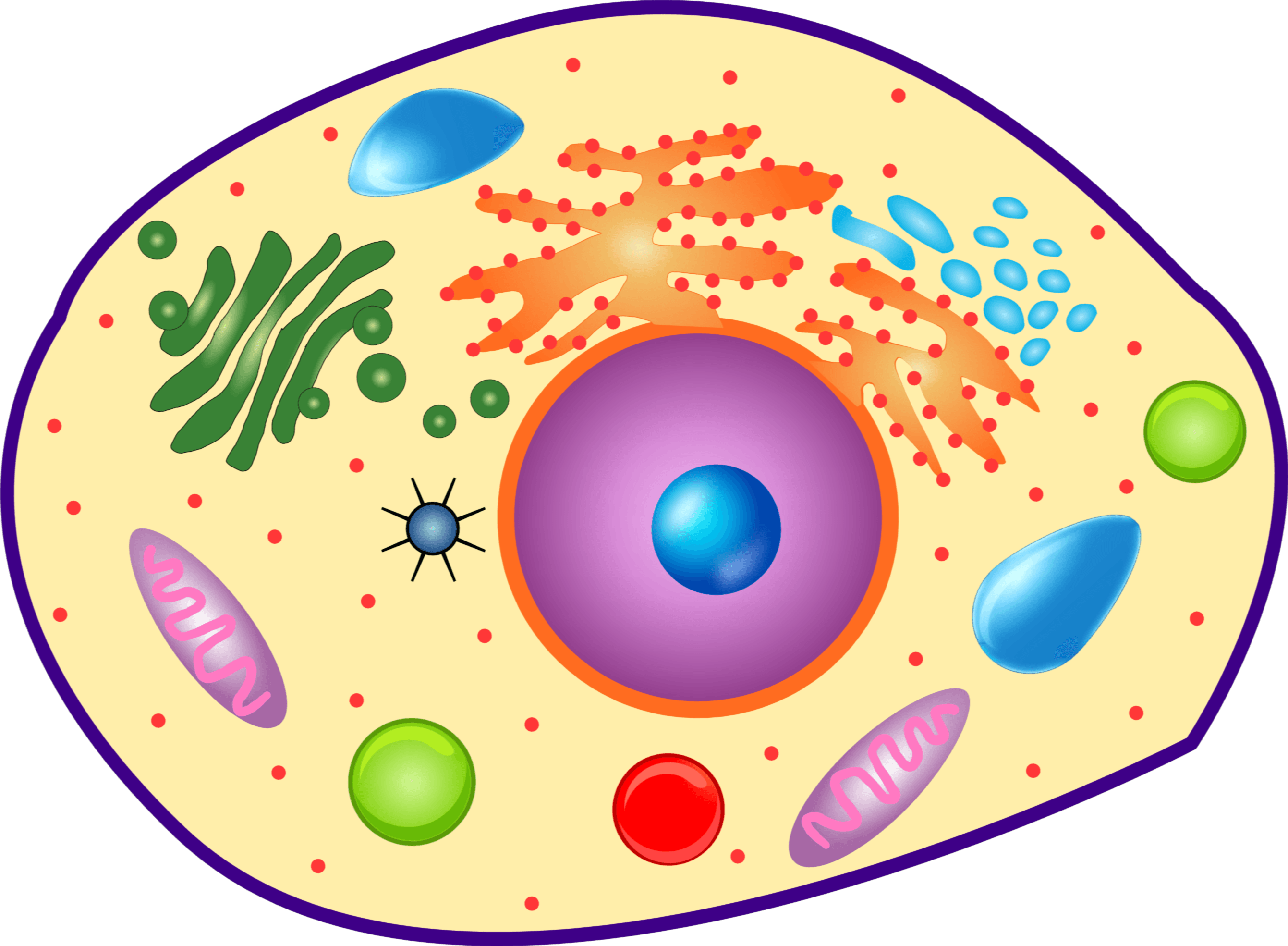
Overview: the cell & its organelles
The eukaryotic cell compartmentalises its work. The nucleus stores DNA and is the site of transcription; the rough endoplasmic reticulum, studded with ribosomes, synthesises secreted and membrane proteins; the smooth ER handles lipids and calcium; the Golgi apparatus modifies, sorts and packages proteins; mitochondria generate ATP and release factors that trigger intrinsic apoptosis; and lysosomes degrade material with acid hydrolases. In musculoskeletal tissue these are specialised: chondrocytes and osteoblasts have prominent rough ER and Golgi to manufacture and secrete the collagen-rich extracellular matrix, while the osteoclast is a multinucleated cell that resorbs bone using lysosomal enzymes (and acid) delivered at its ruffled border.
A cell-biology primer for orthopaedics needs the mesenchymal stem/stromal cell (MSC) — the multipotent progenitor of the musculoskeletal lineages:
- Sources: bone marrow (the classic), periosteum, adipose tissue, muscle and synovium.
- Trilineage differentiation: the defining capacity to become osteoblast, chondrocyte and adipocyte (also tenocyte/myocyte).
- Master lineage transcription factors: Runx2 (with Osterix/SP7) drives the osteoblast line, Sox9 the chondrocyte line, and PPAR-gamma the adipocyte line — competing programmes from one progenitor (the osteoblast-vs-adipocyte switch matters in ageing/osteoporosis).
- Identity (ISCT criteria): plastic-adherent, trilineage-capable, surface markers positive for CD73/CD90/CD105 and negative for haematopoietic markers (CD34/CD45).
- Why orthopaedics cares: periosteal and marrow MSCs are the cellular engine of fracture healing, the osteogenic component of bone grafts, and the basis of cartilage/tendon repair and cell therapy - all developed on stem cells and MSCs in orthopaedics.
The cell cycle
Dividing cells progress through interphase — G1 (growth), S (DNA synthesis/replication), G2 (growth/preparation) — and then M (mitosis); non-dividing cells rest in G0. Progression is driven by cyclins and cyclin-dependent kinases (CDKs) and policed at checkpoints (principally G1/S and G2/M) that verify DNA integrity and replication before the cell commits. The tumour suppressors p53 (the "guardian of the genome", which arrests the cycle or triggers apoptosis when DNA is damaged) and Rb are central. Loss of cell-cycle control — through oncogene activation or tumour-suppressor loss — is the basis of oncogenesis, relevant to bone and soft-tissue tumours.
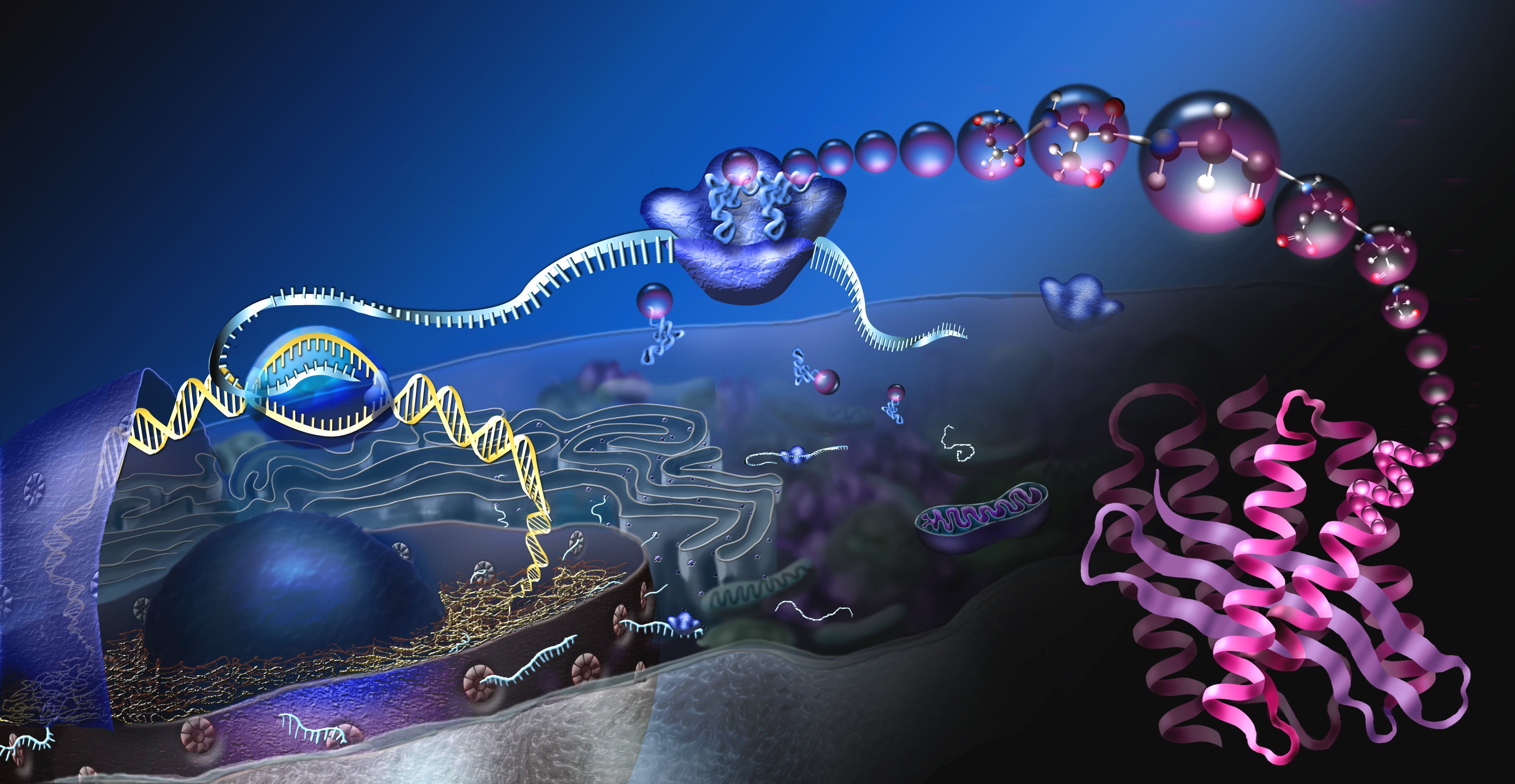
Concepts: the central dogma
Genetic information flows DNA → RNA → protein. In the nucleus, a gene's DNA is transcribed by RNA polymerase into messenger RNA (mRNA), which is processed (splicing, capping, poly-A tail) and exported to the cytoplasm. There, ribosomes translate the mRNA codons into a chain of amino acids, using transfer RNA. The polypeptide then folds and undergoes post-translational modification into a functional protein. A mutation at any point yields an abnormal protein and disease — the molecular basis of many orthopaedic conditions: COL1A1/COL1A2 (osteogenesis imperfecta), FGFR3 (achondroplasia), COMP (pseudoachondroplasia/MED), EXT1/2 (multiple hereditary exostoses).
The dogma gives the flow; these techniques interrogate each step and are examinable basic science:
- DNA: PCR amplifies a target sequence (qPCR quantifies; RT-PCR starts from RNA); the Southern blot detects a DNA sequence; Sanger and next-generation sequencing (NGS) read the sequence (sarcoma gene panels, germline dysplasia testing).
- RNA: the Northern blot and RT-qPCR measure gene expression.
- Protein: the Western blot (size-separated, antibody-detected), ELISA (quantifies a protein/antibody), and immunohistochemistry (IHC) (localises a protein in a tissue section — tumour markers). (Blot mnemonic: SNoW DRoP — Southern=DNA, Northern=RNA, Western=Protein.)
- Cytogenetics: the karyotype and FISH detect translocations/amplifications.
- Orthopaedic applications: detecting sarcoma fusion genes (e.g. EWSR1–FLI1 in Ewing sarcoma by RT-PCR / FISH break-apart; SS18–SSX in synovial sarcoma; MDM2 amplification in atypical lipomatous tumour / parosteal osteosarcoma by FISH), IHC markers (CD99 in Ewing, SATB2 for osteoblastic lesions), and broad-range 16S rRNA PCR for organism detection in culture-negative prosthetic joint infection. The two fusion-gene examples have their own pages - Ewing sarcoma and synovial sarcoma - and are worth reading beside this section, because they are where an abstract assay becomes the thing that names the tumour.
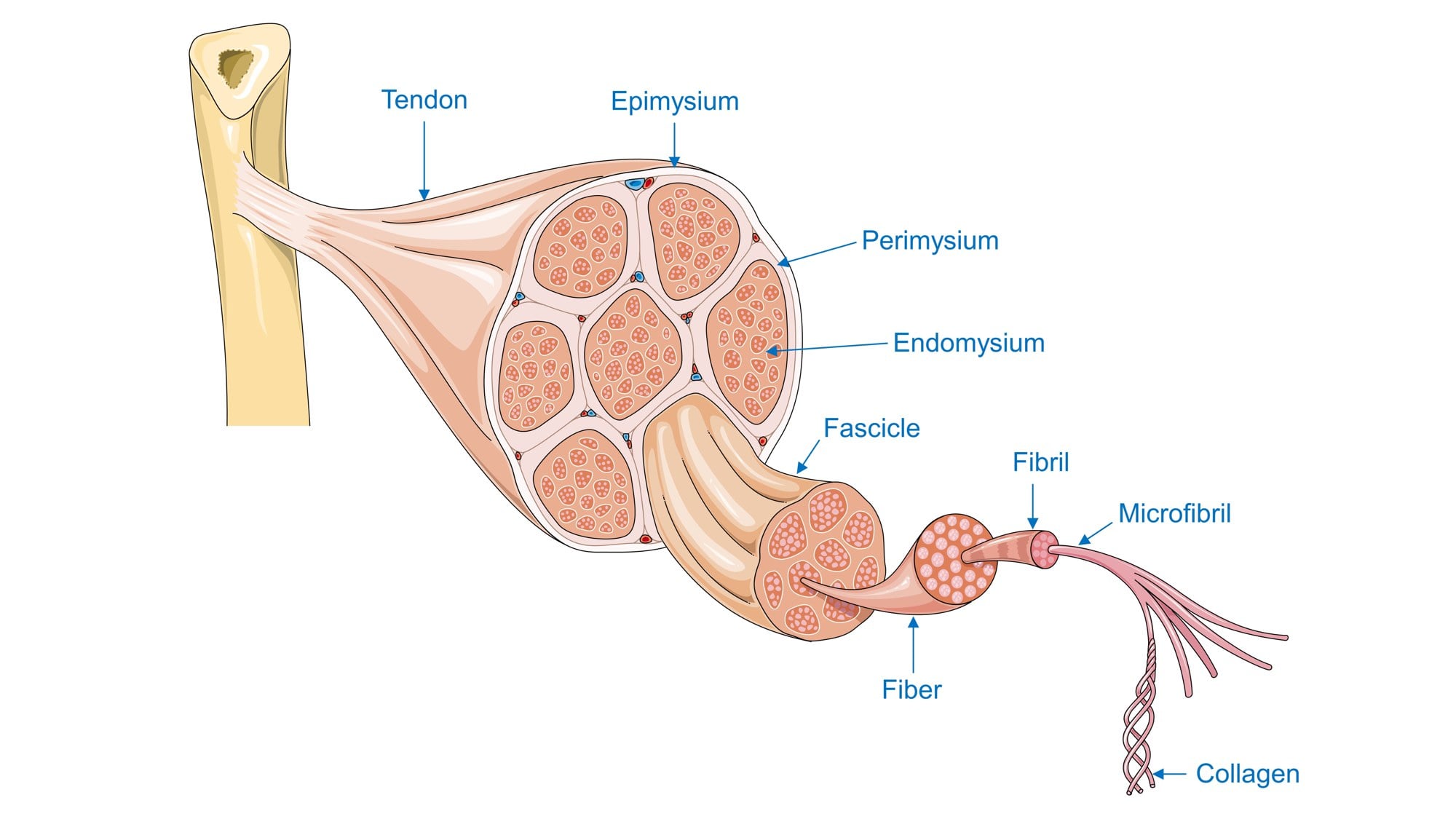
Collagen — the orthopaedic protein
Collagen is the dominant structural protein of the musculoskeletal system and the best orthopaedic example of protein synthesis and post-translational modification:
- Transcription/translation of pro-alpha chains on the rough ER, each with the repeating glycine-X-Y sequence (X often proline, Y often hydroxyproline).
- Hydroxylation of proline and lysine residues — which requires VITAMIN C as a cofactor. Its lack is scurvy, where the failure is at THIS single step: the chains are made but cannot be stabilised, so what is secreted is under-hydroxylated and mechanically useless - which is why the disease shows up as bleeding, poor healing and, in the child, a radiographically distinctive metaphysis.
- Glycosylation and assembly of three chains into the triple helix (procollagen).
- Secretion, then cleavage of the propeptides to form tropocollagen.
- Fibril assembly and CROSS-LINKING (lysyl oxidase) for tensile strength.
There are 28 collagen types; the fibrillar collagens (types I, II, III, V, XI...) build the load-bearing frameworks. Type I predominates in bone, tendon and skin; type II in hyaline cartilage.
- Main location
- Bone, tendon, ligament, skin, annulus fibrosus
- Note
- Most abundant; defective in osteogenesis imperfecta
- Main location
- Hyaline (articular) cartilage, nucleus pulposus
- Note
- Cartilage; defective in some chondrodysplasias
- Main location
- Early wound/granulation tissue, vessels
- Note
- Laid down early in healing, later replaced by type I
- Main location
- Regulate fibril diameter (with I / II)
- Note
- Co-assemble with the major fibrillar collagens
- Main location
- Hypertrophic zone of the growth plate
- Note
- Marker of hypertrophic chondrocytes (endochondral ossification)
Clinical relevance: cell death & cell signalling
Active, ATP-dependent, regulated cell death: cell shrinkage, chromatin condensation, membrane blebbing, apoptotic bodies cleared by phagocytes — NO inflammation. Via the intrinsic (mitochondrial, Bcl-2 family/cytochrome c) and extrinsic (death-receptor, e.g. Fas) pathways converging on caspases. Physiological (e.g. growth-plate hypertrophic chondrocytes); dysregulated chondrocyte apoptosis contributes to osteoarthritis.
Passive, unregulated death from injury/ischaemia: cell swelling, membrane rupture, spillage of contents → INFLAMMATION. Seen in infarction and osteonecrosis - avascular necrosis of the hip is the clinical archetype - and in severe trauma and infection.
Cells coordinate via chemical signals classified by range: endocrine (hormones via the bloodstream, e.g. PTH, oestrogen), paracrine (local diffusion to neighbours, e.g. growth factors in fracture healing), autocrine (a cell signalling itself), and juxtacrine/direct contact (e.g. Notch). Signals bind receptors (cell-surface or intracellular) and trigger intracellular cascades (second messengers, kinases, transcription factors) that change gene expression — the machinery behind the bone-signalling pathways (Wnt, RANK–RANKL–OPG, BMP/TGF-beta, Hedgehog, Notch).
Mnemonics & memory aids
COLLAGENCollagen synthesis
Hook:COLLAGEN: chains, Gly-X-Y, vitamin-C hydroxylation, triple helix, cross-linking — type I bone, type II cartilage.
APOPTOSISApoptosis vs necrosis
Hook:APOPTOSIS is active, orderly and caspase-driven with no inflammation — necrosis is the messy, inflammatory opposite.
Viva practice
Exam viva
Practise clinical reasoning and management decisions out loud
“Walk me through the central dogma and use collagen to illustrate how a protein is made and modified. Why is vitamin C relevant?”
“Distinguish apoptosis from necrosis, and give orthopaedic examples of each. How do cells signal to one another?”
Exam cheat sheet
Organelles (ortho roles)
- Nucleus = DNA/transcription; rough ER + ribosomes = protein synthesis (collagen)
- Golgi = modify/package; mitochondria = ATP + intrinsic apoptosis
- Lysosomes = degradation (osteoclast bone resorption)
Cell cycle & central dogma
- G1 → S → G2 → M; checkpoints (G1/S, G2/M); cyclins/CDKs; p53 & Rb
- DNA → mRNA (transcription) → protein (translation)
- Mutations → disease: COL1A1 (OI), FGFR3 (achondroplasia), COMP (pseudoachondroplasia)
Collagen
- Gly-X-Y triple helix; prolyl/lysyl hydroxylation needs VITAMIN C (scurvy)
- Procollagen → secreted → cleaved → fibril → cross-linked (lysyl oxidase)
- Type I bone/tendon, II cartilage, III early healing, X hypertrophic physis
Cell death & signalling
- Apoptosis: programmed, ATP-dependent, caspases, NO inflammation (intrinsic + extrinsic)
- Necrosis: passive, swelling/lysis, inflammation (osteonecrosis, infarction)
- Signalling: endocrine / paracrine (fracture healing) / autocrine / juxtacrine
Evidence Base
Fibrillar collagens
- The fibrillar collagens (types I, II, III, V, XI, XXIV, XXVII) provide three-dimensional frameworks conferring mechanical strength; humans have 28 collagen types.
- The triple-helix structure depends on the amino-acid sequence (Gly-X-Y), hydrogen bonding and post-translational modifications such as prolyl 4-hydroxylation.
- Biosynthesis involves prolyl/lysyl hydroxylation, chaperones, trimerisation of procollagen, proteolytic maturation, fibril assembly and cross-linking.
Osteogenesis imperfecta
- Osteogenesis imperfecta is caused by dominant COL1A1/COL1A2 mutations in about 85% of individuals, affecting type I collagen quantity or structure - the central-dogma 'gene to protein to disease' exemplar.
- Many additional (mostly recessive) defects affect proteins of type I collagen synthesis, processing, secretion and post-translational modification, or bone-cell differentiation/activity.
- Phenotype extends beyond bone (cardiovascular, pulmonary, skin, hearing, dentinogenesis imperfecta); management is surgical + medical, with gene/cell and signalling therapies under study.
The role of apoptosis in the pathogenesis of osteoarthritis
- Apoptosis is an important physiological process for development and tissue homeostasis; dysregulated chondrocyte apoptosis contributes to osteoarthritis (cartilage degeneration).
- Inflammatory mediators (ROS, NO, IL-1beta, TNF-alpha, Fas) and signalling pathways (NF-kappaB, Wnt, Notch) drive chondrocyte apoptosis and matrix degradation.
- Connects core cell-death biology directly to a common orthopaedic disease and to potential therapeutic targets.
The collagen structure/biosynthesis facts come from Bella & Hulmes 2017 (DOI); the central-dogma-to-disease exemplar (COL1A1/COL1A2 in ~85% of osteogenesis imperfecta) from Marini et al. 2017 (DOI); and the apoptosis-in-OA links from Xiao et al. 2023 (DOI). The general cell-biology content (organelles, cell cycle, central dogma) is standard textbook science. The disease links are each developed on their own page, and this primer exists to make them make sense: osteogenesis imperfecta is the COL1A1/COL1A2 fault worked all the way through to brittle bone, achondroplasia the FGFR3 one, pseudoachondroplasia the COMP one, and multiple hereditary exostoses the EXT1/EXT2 one - all four sitting under skeletal dysplasias. The signalling cascades sketched above are set out in full in bone signalling pathways.